Related Research Articles

The Frank–Starling law of the heart represents the relationship between stroke volume and end diastolic volume. The law states that the stroke volume of the heart increases in response to an increase in the volume of blood in the ventricles, before contraction, when all other factors remain constant. As a larger volume of blood flows into the ventricle, the blood stretches cardiac muscle, leading to an increase in the force of contraction. The Frank-Starling mechanism allows the cardiac output to be synchronized with the venous return, arterial blood supply and humoral length, without depending upon external regulation to make alterations. The physiological importance of the mechanism lies mainly in maintaining left and right ventricular output equality.

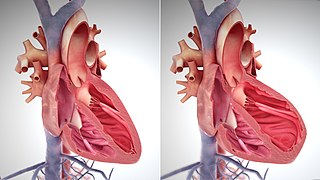
Diastole is the relaxed phase of the cardiac cycle when the chambers of the heart are re-filling with blood. The contrasting phase is systole when the heart chambers are contracting. Atrial diastole is the relaxing of the atria, and ventricular diastole the relaxing of the ventricles.

Atrial septal defect (ASD) is a congenital heart defect in which blood flows between the atria of the heart. Some flow is a normal condition both pre-birth and immediately post-birth via the foramen ovale; however, when this does not naturally close after birth it is referred to as a patent (open) foramen ovale (PFO). It is common in patients with a congenital atrial septal aneurysm (ASA).

The jugular venous pressure is the indirectly observed pressure over the venous system via visualization of the internal jugular vein. It can be useful in the differentiation of different forms of heart and lung disease. Classically three upward deflections and two downward deflections have been described.

Cardiac catheterization is the insertion of a catheter into a chamber or vessel of the heart. This is done both for diagnostic and interventional purposes.

The atrium is one of the two upper chambers in the heart that receives blood from the circulatory system. The blood in the atria is pumped into the heart ventricles through the atrioventricular mitral and tricuspid heart valves.
In cardiac physiology, preload is the amount of sarcomere stretch experienced by cardiac muscle cells, called cardiomyocytes, at the end of ventricular filling during diastole. Preload is directly related to ventricular filling. As the relaxed ventricle fills during diastole, the walls are stretched and the length of sarcomeres increases. Sarcomere length can be approximated by the volume of the ventricle because each shape has a conserved surface-area-to-volume ratio. This is useful clinically because measuring the sarcomere length is destructive to heart tissue. It requires cutting out a piece of cardiac muscle to look at the sarcomeres under a microscope. It is currently not possible to directly measure preload in the beating heart of a living animal. Preload is estimated from end-diastolic ventricular pressure and is measured in millimeters of mercury (mmHg).

The cardiac cycle is the performance of the human heart from the beginning of one heartbeat to the beginning of the next. It consists of two periods: one during which the heart muscle relaxes and refills with blood, called diastole, following a period of robust contraction and pumping of blood, called systole. After emptying, the heart relaxes and expands to receive another influx of blood returning from the lungs and other systems of the body, before again contracting to pump blood to the lungs and those systems. A normally performing heart must be fully expanded before it can efficiently pump again. Assuming a healthy heart and a typical rate of 70 to 75 beats per minute, each cardiac cycle, or heartbeat, takes about 0.8 second to complete the cycle. There are two atrial and two ventricle chambers of the heart; they are paired as the left heart and the right heart—that is, the left atrium with the left ventricle, the right atrium with the right ventricle—and they work in concert to repeat the cardiac cycle continuously. At the start of the cycle, during ventricular diastole–early, the heart relaxes and expands while receiving blood into both ventricles through both atria; then, near the end of ventricular diastole–late, the two atria begin to contract, and each atrium pumps blood into the ventricle below it. During ventricular systole the ventricles are contracting and vigorously pulsing two separated blood supplies from the heart—one to the lungs and one to all other body organs and systems—while the two atria are relaxed. This precise coordination ensures that blood is efficiently collected and circulated throughout the body.
Pulsus paradoxus, also paradoxic pulse or paradoxical pulse, is an abnormally large decrease in stroke volume, systolic blood pressure and pulse wave amplitude during inspiration. Pulsus paradoxus is not related to pulse rate or heart rate, and it is not a paradoxical rise in systolic pressure. Normally, blood pressure drops less precipitously than 10 mmHg during inhalation. Pulsus paradoxus is a sign that is indicative of several conditions most commonly pericardial effusion.
Central venous pressure (CVP) is the blood pressure in the venae cavae, near the right atrium of the heart. CVP reflects the amount of blood returning to the heart and the ability of the heart to pump the blood back into the arterial system. CVP is often a good approximation of right atrial pressure (RAP), although the two terms are not identical, as a pressure differential can sometimes exist between the venae cavae and the right atrium. CVP and RAP can differ when arterial tone is altered. This can be graphically depicted as changes in the slope of the venous return plotted against right atrial pressure.
The Bainbridge reflex or Bainbridge effect, also called the atrial reflex, is an increase in heart rate due to an increase in central venous pressure. Increased blood volume is detected by stretch receptors located in both sides of atria at the venoatrial junctions.
Venous return is the rate of blood flow back to the heart. It normally limits cardiac output.
Right atrial pressure (RAP) is the blood pressure in the right atrium of the heart. RAP reflects the amount of blood returning to the heart and the ability of the heart to pump the blood into the arterial system. RAP is often nearly identical to central venous pressure (CVP), although the two terms are not identical, as a pressure differential can sometimes exist between the venae cavae and the right atrium. CVP and RAP can differ when venous tone is altered. This can be graphically depicted as changes in the slope of the venous return plotted against right atrial pressure.

Volume overload refers to the state of one of the chambers of the heart in which too large a volume of blood exists within it for it to function efficiently. Ventricular volume overload is approximately equivalent to an excessively high preload. It is a cause of cardiac failure.
In medicine, the mean systemic pressure is defined as the mean pressure that exists in the circulatory system when there is no blood motion. A similar term, mean circulatory filling pressure, (MCFP) is defined as the mean pressure that exists in the combined circulatory system & pulmonary system when there is no blood motion. The value of MSP in animal experimental models is approximately 7 mm Hg. It is an indicator of how full the circulatory system is, and is influenced by the volume of circulating blood and the smooth muscle tone in the walls of the venous system .
Low pressure baroreceptors are baroreceptors that relay information derived from blood pressure within the autonomic nervous system. They are stimulated by stretching of the vessel wall. They are located in large systemic veins and in the walls of the atria of the heart, and pulmonary vasculature. Low pressure baroreceptors are also referred to as volume receptors and cardiopulmonary baroreceptors.
Cardiac physiology or heart function is the study of healthy, unimpaired function of the heart: involving blood flow; myocardium structure; the electrical conduction system of the heart; the cardiac cycle and cardiac output and how these interact and depend on one another.
A plot of a system's pressure versus volume has long been used to measure the work done by the system and its efficiency. This analysis can be applied to heat engines and pumps, including the heart. A considerable amount of information on cardiac performance can be determined from the pressure vs. volume plot. A number of methods have been determined for measuring PV-loop values experimentally.

Heart failure with preserved ejection fraction (HFpEF) is a form of heart failure in which the ejection fraction – the percentage of the volume of blood ejected from the left ventricle with each heartbeat divided by the volume of blood when the left ventricle is maximally filled – is normal, defined as greater than 50%; this may be measured by echocardiography or cardiac catheterization. Approximately half of people with heart failure have preserved ejection fraction, while the other half have a reduction in ejection fraction, called heart failure with reduced ejection fraction (HFrEF).
The main pathophysiology of heart failure is a reduction in the efficiency of the heart muscle, through damage or overloading. As such, it can be caused by a wide number of conditions, including myocardial infarction, hypertension and cardiac amyloidosis. Over time these increases in workload will produce changes to the heart itself:
References
- ↑ Brengelmann GL (March 2003). "A critical analysis of the view that right atrial pressure determines venous return". J. Appl. Physiol. 94 (3): 849–59. doi:10.1152/japplphysiol.00868.2002. PMID 12391065.
- ↑ "Cardiac Basic Physiology". Archived from the original on 2008-10-11.