In cellular biology, active transport is the movement of molecules or ions across a cell membrane from a region of lower concentration to a region of higher concentration—against the concentration gradient. Active transport requires cellular energy to achieve this movement. There are two types of active transport: primary active transport that uses adenosine triphosphate (ATP), and secondary active transport that uses an electrochemical gradient. This process is in contrast to passive transport, which allows molecules or ions to move down their concentration gradient, from an area of high concentration to an area of low concentration, without energy.

Amiloride, sold under the trade name Midamor among others, is a medication typically used with other medications to treat high blood pressure or swelling due to heart failure or cirrhosis of the liver. Amiloride is classified as a potassium-sparing diuretic. Amiloride is often used together with another diuretic, such as a thiazide or loop diuretic. It is taken by mouth. Onset of action is about two hours and it lasts for about a day.

Thiazide refers to both a class of sulfur-containing organic molecules and a class of diuretics based on the chemical structure of benzothiadiazine. The thiazide drug class was discovered and developed at Merck and Co. in the 1950s. The first approved drug of this class, chlorothiazide, was marketed under the trade name Diuril beginning in 1958. In most countries, thiazides are the least expensive antihypertensive drugs available.

Diabetic nephropathy, also known as diabetic kidney disease, is the chronic loss of kidney function occurring in those with diabetes mellitus. Diabetic nephropathy is the leading causes of chronic kidney disease (CKD) and end-stage renal disease (ESRD) globally. The triad of protein leaking into the urine, rising blood pressure with hypertension and then falling renal function is common to many forms of CKD. Protein loss in the urine due to damage of the glomeruli may become massive, and cause a low serum albumin with resulting generalized body swelling (edema) so called nephrotic syndrome. Likewise, the estimated glomerular filtration rate (eGFR) may progressively fall from a normal of over 90 ml/min/1.73m2 to less than 15, at which point the patient is said to have end-stage renal disease. It usually is slowly progressive over years.

Glycosuria is the excretion of glucose into the urine. Ordinarily, urine contains no glucose because the kidneys are able to reabsorb all of the filtered glucose from the tubular fluid back into the bloodstream. Glycosuria is nearly always caused by elevated blood glucose levels, most commonly due to untreated diabetes mellitus. Rarely, glycosuria is due to an intrinsic problem with glucose reabsorption within the kidneys, producing a condition termed renal glycosuria. Glycosuria leads to excessive water loss into the urine with resultant dehydration, a process called osmotic diuresis.
Sodium-dependent glucose cotransporters are a family of glucose transporter found in the intestinal mucosa (enterocytes) of the small intestine (SGLT1) and the proximal tubule of the nephron. They contribute to renal glucose reabsorption. In the kidneys, 100% of the filtered glucose in the glomerulus has to be reabsorbed along the nephron. If the plasma glucose concentration is too high (hyperglycemia), glucose passes into the urine (glucosuria) because SGLT are saturated with the filtered glucose.
Renal glycosuria is a rare condition in which the simple sugar glucose is excreted in the urine despite normal or low blood glucose levels. With normal kidney (renal) function, glucose is excreted in the urine only when there are abnormally elevated levels of glucose in the blood. However, in those with renal glycosuria, glucose is abnormally elevated in the urine due to improper functioning of the renal tubules, which are primary components of nephrons, the filtering units of the kidneys.

The sodium/glucose cotransporter 2 (SGLT2) is a protein that in humans is encoded by the SLC5A2 gene.
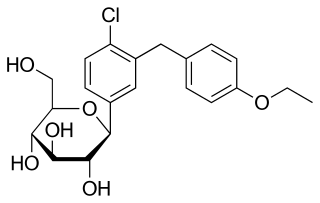
Dapagliflozin, sold under the brand names Farxiga (US) and Forxiga (EU) among others, is a medication used to treat type 2 diabetes. It is also used to treat adults with heart failure and chronic kidney disease.
Renal glucose reabsorption is the part of kidney (renal) physiology that deals with the retrieval of filtered glucose, preventing it from disappearing from the body through the urine.
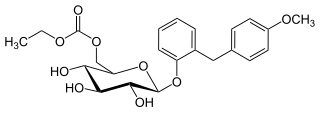
Sergliflozin etabonate is an investigational anti-diabetic drug being developed by GlaxoSmithKline. It did not undergo further development after phase II.

Remogliflozin etabonate (INN/USAN) is a drug of the gliflozin class for the treatment of non-alcoholic steatohepatitis ("NASH") and type 2 diabetes. Remogliflozin was discovered by the Japanese company Kissei Pharmaceutical and is currently being developed by BHV Pharma, a wholly owned subsidiary of North Carolina, US-based Avolynt, and Glenmark Pharmaceuticals through a collaboration with BHV. In 2002, GlaxoSmithKline (GSK) received a license to use it. From 2002 to 2009, GSK carried out a significant clinical development program for the treatment of type-2 diabetes mellitus in various nations across the world and obesity in the UK. Remogliflozin etabonate's pharmacokinetics, pharmacodynamics, and clinical dose regimens were characterized in 18 Phase I and 2 Phase II investigations. Due to financial concerns, GSK stopped working on remogliflozin and sergliflozin, two further SGLT2 inhibitors that were licensed to the company, in 2009. Remogliflozin was commercially launched first in India by Glenmark in May 2019.
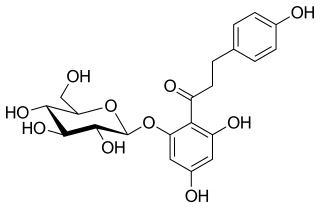
Phlorizin is a glucoside of phloretin, a dihydrochalcone. A white solid, samples often appear yellow owing to impurities. It is of sweet taste and contains four molecules of water in the crystal. Above 200 °C, it decomposes to give rufin. It is poorly soluble in ether and cold water, but soluble in ethanol and hot water. Upon prolonged exposure to aqueous solutions phlorizin hydrolyzes to phloretin and glucose.

Canagliflozin, sold under the brand name Invokana among others, is a medication used to treat type 2 diabetes. It is used together with exercise and diet. It is not recommended in type 1 diabetes. It is taken by mouth.
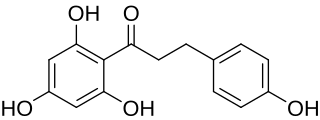
Phloretin is a dihydrochalcone, a type of natural phenol. It can be found in apple tree leaves and the Manchurian apricot.
Empagliflozin, sold under the brand name Jardiance, among others, is an antidiabetic medication used to improve glucose control in people with type 2 diabetes. It is not recommended for type 1 diabetes. It is taken by mouth.

Tofogliflozin is an experimental drug for the treatment of diabetes mellitus and is being developed by Chugai Pharma in collaboration with Kowa and Sanofi. It is an inhibitor of subtype 2 sodium-glucose transport protein (SGLT2), which is responsible for at least 90% of the glucose reabsorption in the kidney. As of September 2012, the drug is in Phase III clinical trials.
SGLT2 inhibitors, also called gliflozins or flozins, are a class of medications that modulate sodium-glucose transport proteins in the nephron, unlike SGLT1 inhibitors that perform a similar function in the intestinal mucosa. The foremost metabolic effect of this is to inhibit reabsorption of glucose in the kidney and therefore lower blood sugar. They act by inhibiting sodium-glucose transport protein 2 (SGLT2). SGLT2 inhibitors are used in the treatment of type II diabetes mellitus (T2DM). Apart from blood sugar control, gliflozins have been shown to provide significant cardiovascular benefit in patients with type II diabetes (T2DM). Several medications of this class have been approved or are currently under development. In studies on canagliflozin, a member of this class, the medication was found to enhance blood sugar control as well as reduce body weight and systolic and diastolic blood pressure.
Sotagliflozin, sold under the brand name Inpefa among others, is a medication used to reduce the risk of death due to heart failure.
Canagliflozin/metformin, sold under the brand name Vokanamet among others, is a fixed-dose combination anti-diabetic medication used for the treatment of type 2 diabetes. It is used in combination with diet and exercise. It is taken by mouth.








