Time between a new disease's identification and first diagnoses
Lead time bias occurs if testing increases the perceived survival time without affecting the course of the disease.
Lead time bias happens when survival time appears longer because diagnosis was done earlier (for instance, by screening), irrespective of whether the patient lived longer. Lead time is the duration of time between the detection of a disease (by screening or based on new experimental criteria) and its usual clinical presentation and diagnosis (based on traditional criteria).[1] For example, it is the time between early detection by screening and the time when diagnosis would have been made clinically (without screening).[1] It is an important factor when evaluating the effectiveness of a specific test.[2]
The goal of screening is earlier detection (to diagnose a disease earlier than it would be without screening). Therefore, if screening works, it needs to advance in time to the moment of diagnosis. In other words, screening needs to introduce a lead time. However, the lead time itself biases survival statistics: people with diseases detected by screening appear to have a longer survival (the time the person has lived after diagnosis) only because screening starts the clock sooner.[citation needed]
Consider, for instance, a disease where there is no screening that is diagnosed by symptoms when patients are 60 years old and kills them when they are 65 years old. These patients lived 5 years after the diagnosis. Now, consider that with screening, the disease is detected when the patients are 55 years old, but they still die when they are 65. They did not live any longer because of earlier detection, but they survived 10 years after the diagnosis (only because the disease was diagnosed 5 years earlier). Therefore, earlier detection alone is not enough to achieve longer survival.[citation needed]
Lead time bias affects the interpretation of the five-year survival rate, effectively making it appear that people survive longer with cancer even in cases where the course of cancer is the same as in those who were diagnosed later.[3]
Another example is when early diagnosis by screening may not prolong the life of someone but just determine the propensity of the person to a disease or medical condition, such as by DNA testing.[1] No additional life span has been gained, and the patient may even be subject to added anxiety as the patient must live for longer with knowledge of the disease. For example, the genetic disorderHuntington's disease is diagnosed when symptoms appear at around 50, and the person dies at around 65. The typical patient, therefore, lives about 15 years after diagnosis. A genetic test at birth makes it possible to diagnose this disorder earlier. If this newborn baby dies at around 65, the person will have "survived" 65 years after diagnosis, without having actually lived any longer than those diagnosed without DNA detection.[citation needed]
Colorectal cancer (CRC), also known as bowel cancer, colon cancer, or rectal cancer, is the development of cancer from the colon or rectum. Signs and symptoms may include blood in the stool, a change in bowel movements, weight loss, abdominal pain and fatigue. Most colorectal cancers are due to old age and lifestyle factors, with only a small number of cases due to underlying genetic disorders. Risk factors include diet, obesity, smoking, and lack of physical activity. Dietary factors that increase the risk include red meat, processed meat, and alcohol. Another risk factor is inflammatory bowel disease, which includes Crohn's disease and ulcerative colitis. Some of the inherited genetic disorders that can cause colorectal cancer include familial adenomatous polyposis and hereditary non-polyposis colon cancer; however, these represent less than 5% of cases. It typically starts as a benign tumor, often in the form of a polyp, which over time becomes cancerous.
Hepatocellular carcinoma (HCC) is the most common type of primary liver cancer in adults and is currently the most common cause of death in people with cirrhosis. HCC is the third leading cause of cancer-related deaths worldwide.
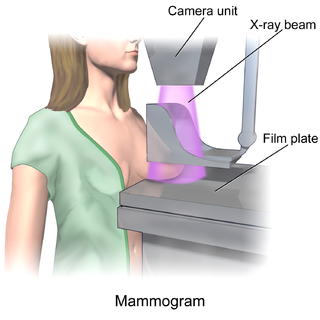
Mammography is the process of using low-energy X-rays to examine the human breast for diagnosis and screening. The goal of mammography is the early detection of breast cancer, typically through detection of characteristic masses or microcalcifications.
Pancreatic cancer arises when cells in the pancreas, a glandular organ behind the stomach, begin to multiply out of control and form a mass. These cancerous cells have the ability to invade other parts of the body. A number of types of pancreatic cancer are known.
Ovarian cancer is a cancerous tumor of an ovary. It may originate from the ovary itself or more commonly from communicating nearby structures such as fallopian tubes or the inner lining of the abdomen. The ovary is made up of three different cell types including epithelial cells, germ cells, and stromal cells. When these cells become abnormal, they have the ability to divide and form tumors. These cells can also invade or spread to other parts of the body. When this process begins, there may be no or only vague symptoms. Symptoms become more noticeable as the cancer progresses. These symptoms may include bloating, vaginal bleeding, pelvic pain, abdominal swelling, constipation, and loss of appetite, among others. Common areas to which the cancer may spread include the lining of the abdomen, lymph nodes, lungs, and liver.
Anal cancer is a cancer which arises from the anus, the distal opening of the gastrointestinal tract. Symptoms may include bleeding from the anus or a lump near the anus. Other symptoms may include pain, itchiness, or discharge from the anus. A change in bowel movements may also occur.
Familial adenomatous polyposis (FAP) is an autosomal dominant inherited condition in which numerous adenomatous polyps form mainly in the epithelium of the large intestine. While these polyps start out benign, malignant transformation into colon cancer occurs when they are left untreated. Three variants are known to exist, FAP and attenuated FAP are caused by APC gene defects on chromosome 5 while autosomal recessive FAP is caused by defects in the MUTYH gene on chromosome 1. Of the three, FAP itself is the most severe and most common; although for all three, the resulting colonic polyps and cancers are initially confined to the colon wall. Detection and removal before metastasis outside the colon can greatly reduce and in many cases eliminate the spread of cancer.
Invasive carcinoma of no special type, invasive breast carcinoma of no special type (IBC-NST), invasive ductal carcinoma (IDC), infiltrating ductal carcinoma (IDC) or invasive ductal carcinoma, not otherwise specified (NOS) is a disease. For international audiences this article will use "invasive carcinoma NST" because it is the preferred term of the World Health Organization (WHO).
Screening, in medicine, is a strategy used to look for as-yet-unrecognised conditions or risk markers. This testing can be applied to individuals or to a whole population without symptoms or signs of the disease being screened.
Overdiagnosis is the diagnosis of disease that will never cause symptoms or death during a patient's ordinarily expected lifetime and thus presents no practical threat regardless of being pathologic. Overdiagnosis is a side effect of screening for early forms of disease. Although screening saves lives in some cases, in others it may turn people into patients unnecessarily and may lead to treatments that do no good and perhaps do harm. Given the tremendous variability that is normal in biology, it is inherent that the more one screens, the more incidental findings will generally be found. For a large percentage of them, the most appropriate medical response is to recognize them as something that does not require intervention; but determining which action a particular finding warrants can be very difficult, whether because the differential diagnosis is uncertain or because the risk ratio is uncertain.
The five-year survival rate is a type of survival rate for estimating the prognosis of a particular disease, normally calculated from the point of diagnosis. Lead time bias from earlier diagnosis can affect interpretation of the five-year survival rate.
Breast cancer screening is the medical screening of asymptomatic, apparently healthy women for breast cancer in an attempt to achieve an earlier diagnosis. The assumption is that early detection will improve outcomes. A number of screening tests have been employed, including clinical and self breast exams, mammography, genetic screening, ultrasound, and magnetic resonance imaging.
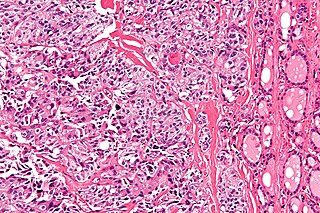
Medullary thyroid cancer is a form of thyroid carcinoma which originates from the parafollicular cells, which produce the hormone calcitonin. Medullary tumors are the third most common of all thyroid cancers and together make up about 3% of all thyroid cancer cases. MTC was first characterized in 1959.
Renal medullary carcinoma is a rare type of cancer that affects the kidney. It tends to be aggressive, difficult to treat, and is often metastatic at the time of diagnosis. Most individuals with this type of cancer have sickle cell trait or rarely sickle cell disease, suggesting that the sickle cell trait may be a risk factor for this type of cancer.
The objective of cancer screening is to detect cancer before symptoms appear, involving various methods such as blood tests, urine tests, DNA tests, and medical imaging. The purpose of screening is early cancer detection, to make the cancer easier to treat and extending life expectancy. In 2019, cancer was the second leading cause of death globally; more recent data is pending due to the COVID-19 pandemic.
A borderline tumor, sometimes called low malignant potential (LMP) tumor, is a distinct but yet heterogeneous group of tumors defined by their histopathology as atypical epithelial proliferation without stromal invasion. It generally refers to such tumors in the ovary but borderline tumors may rarely occur at other locations as well.
Breast cancer awareness is an effort to raise awareness and reduce the stigma of breast cancer through education about screening, symptoms, and treatment. Supporters hope that greater knowledge will lead to earlier detection of breast cancer, which is associated with higher long-term survival rates, and that money raised for breast cancer will produce a reliable, permanent cure.
Active surveillance is a management option for localized prostate cancer that can be offered to appropriate patients who would also be candidates for aggressive local therapies, with the intent to intervene if the disease progresses. Active surveillance should not be confused with watchful waiting, another observational strategy for men that would not be candidates for curative therapy because of a limited life expectancy. Active surveillance offers men with a prostate cancer that is thought to have a low risk of causing harm in the absence of treatment, a chance to delay or avoid aggressive treatment and its associated side effects. While prostate cancer is the most common non-cutaneous cancer and second leading cause of cancer-related death in American men, it is conservatively estimated that approximately 100,000 men per year in the United States who would be eligible for conservative treatment through active surveillance, undergo unnecessary treatments. The management of localized prostate cancer is controversial and men with localized disease diagnosed today often undergo treatments with significant side effects that will not improve overall health outcomes. The 2011 NIH State-of-the-Science Conference Statement on the "Role of active surveillance in the management of men with localized prostate cancer" pointed out the many unanswered questions about observational strategies for prostate cancer that require further research and clarification. These included:
In medicine, breast imaging is a sub-speciality of diagnostic radiology that involves imaging of the breasts for screening or diagnostic purposes. There are various methods of breast imaging using a variety of technologies as described in detail below. Traditional screening and diagnostic mammography uses x-ray technology and has been the mainstay of breast imaging for many decades. Breast tomosynthesis is a relatively new digital x-ray mammography technique that produces multiple image slices of the breast similar to, but distinct from, computed tomography (CT). Xeromammography and galactography are somewhat outdated technologies that also use x-ray technology and are now used infrequently in the detection of breast cancer. Breast ultrasound is another technology employed in diagnosis and screening that can help differentiate between fluid filled and solid lesions, an important factor to determine if a lesion may be cancerous. Breast MRI is a technology typically reserved for high-risk patients and patients recently diagnosed with breast cancer. Lastly, scintimammography is used in a subgroup of patients who have abnormal mammograms or whose screening is not reliable on the basis of using traditional mammography or ultrasound.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.