A nightmare, also known as a bad dream, is an unpleasant dream that can cause a strong emotional response from the mind, typically fear but also despair, anxiety, disgust or sadness. The dream may contain situations of discomfort, psychological or physical terror, or panic. After a nightmare, a person will often awaken in a state of distress and may be unable to return to sleep for a short period of time. Recurrent nightmares may require medical help, as they can interfere with sleeping patterns and cause insomnia.

A sleep disorder, or somnipathy, is a medical disorder of an individual's sleep patterns. Some sleep disorders are severe enough to interfere with normal physical, mental, social and emotional functioning. Sleep disorders are frequent and can have serious consequences on patients' health and quality of life. Polysomnography and actigraphy are tests commonly ordered for diagnosing sleep disorders.
Post-traumatic stress disorder (PTSD) is a mental and behavioral disorder that develops from experiencing a traumatic event, such as sexual assault, warfare, traffic collisions, child abuse, domestic violence, or other threats on a person's life or well-being. Symptoms may include disturbing thoughts, feelings, or dreams related to the events, mental or physical distress to trauma-related cues, attempts to avoid trauma-related cues, alterations in the way a person thinks and feels, and an increase in the fight-or-flight response. These symptoms last for more than a month after the event. Young children are less likely to show distress, but instead may express their memories through play. A person with PTSD is at a higher risk of suicide and intentional self-harm.

Sleep paralysis is a state, during waking up or falling asleep, in which a person is conscious but in a complete state of full-body paralysis. During an episode, the person may hallucinate, which often results in fear. Episodes generally last no more than a few minutes. It can recur multiple times or occur as a single episode.

Night terror, also called sleep terror, is a sleep disorder causing feelings of panic or dread and typically occurring during the first hours of stage 3–4 non-rapid eye movement (NREM) sleep and lasting for 1 to 10 minutes. It can last longer, especially in children. Sleep terror is classified in the category of NREM-related parasomnias in the International Classification of Sleep Disorders. There are two other categories: REM-related parasomnias and other parasomnias. Parasomnias are qualified as undesirable physical events or experiences that occur during entry into sleep, during sleep, or during arousal from sleep.
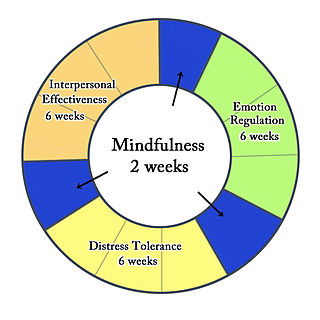
Dialectical behavior therapy (DBT) is an evidence-based psychotherapy that began with efforts to treat personality disorders and interpersonal conflicts. Evidence suggests that DBT can be useful in treating mood disorders and suicidal ideation as well as for changing behavioral patterns such as self-harm and substance use. DBT evolved into a process in which the therapist and client work with acceptance and change-oriented strategies and ultimately balance and synthesize them—comparable to the philosophical dialectical process of thesis and antithesis, followed by synthesis.
Eye movement desensitization and reprocessing (EMDR) is a form of psychotherapy that is controversial within the psychological community. It was devised by Francine Shapiro in 1987 and originally designed to alleviate the distress associated with traumatic memories such as post-traumatic stress disorder (PTSD).

Prazosin, sold under the brand name Minipress among others, is a medication used to treat high blood pressure, symptoms of an enlarged prostate, and nightmares related to post-traumatic stress disorder (PTSD). It is an α1 blocker. It is a less preferred treatment of high blood pressure. Other uses may include heart failure and Raynaud syndrome. It is taken by mouth.
Alpha-1 blockers constitute a variety of drugs that block the effect of catecholamines on alpha-1-adrenergic receptors. They are mainly used to treat benign prostatic hyperplasia (BPH), hypertension and post-traumatic stress disorder. Alpha-1 adrenergic receptors are present in vascular smooth muscle, the central nervous system, and other tissues. When alpha blockers bind to these receptors in vascular smooth muscle, they cause vasodilation.
Complex post-traumatic stress disorder is a stress-related mental disorder generally occurring in response to complex traumas, i.e., commonly prolonged or repetitive exposures to a series of traumatic events, within which individuals perceive little or no chance to escape.
Parasomnias are a category of sleep disorders that involve abnormal movements, behaviors, emotions, perceptions, and dreams that occur while falling asleep, sleeping, between sleep stages, or during arousal from sleep. Parasomnias are dissociated sleep states which are partial arousals during the transitions between wakefulness, NREM sleep, and REM sleep, and their combinations.

Catathrenia or nocturnal groaning is a sleep-related breathing disorder, consisting of end-inspiratory apnea and expiratory groaning during sleep. It describes a rare condition characterized by monotonous, irregular groans while sleeping. Catathrenia begins with a deep inspiration. The person with catathrenia holds her or his breath against a closed glottis, similar to the Valsalva maneuver. Expiration can be slow and accompanied by sound caused by vibration of the vocal cords or a simple rapid exhalation. Despite a slower breathing rate, no oxygen desaturation usually occurs. The moaning sound is usually not noticed by the person producing the sound, but it can be extremely disturbing to sleep partners. It appears more often during expiration REM sleep than in NREM sleep.
A sympatholytic (sympathoplegic) drug is a medication that opposes the downstream effects of postganglionic nerve firing in effector organs innervated by the sympathetic nervous system (SNS). They are indicated for various functions; for example, they may be used as antihypertensives. They are also used to treat anxiety, such as generalized anxiety disorder, panic disorder and PTSD. In some cases, such as with guanfacine, they have also shown to be beneficial in the treatment of ADHD.
Prolonged exposure therapy (PE) is a form of behavior therapy and cognitive behavioral therapy designed to treat post-traumatic stress disorder. It is characterized by two main treatment procedures – imaginal and in vivo exposures. Imaginal exposure is repeated 'on-purpose' retelling of the trauma memory. In vivo exposure is gradually confronting situations, places, and things that are reminders of the trauma or feel dangerous. Additional procedures include processing of the trauma memory and breathing retraining.
Idiopathic hypersomnia(IH) is a neurological disorder which is characterized primarily by excessive sleep and excessive daytime sleepiness (EDS). Idiopathic hypersomnia was first described by Bedrich Roth in 1976, and it can be divided into two forms: polysymptomatic and monosymptomatic. The condition typically becomes evident in early adulthood and most patients diagnosed with IH will have had the disorder for many years prior to their diagnosis. As of August 2021, an FDA-approved medication exists for IH called Xywav, which is oral solution of calcium, magnesium, potassium, and sodium oxybates; in addition to several off-label treatments (primarily FDA-approved narcolepsy medications).
Cognitive behavioral therapy for insomnia (CBT-I) is a technique for treating insomnia without medications. Insomnia is a common problem involving trouble falling asleep, staying asleep, or getting quality sleep. CBT-I aims to improve sleep habits and behaviors by identifying and changing the thoughts and the behaviors that affect the ability of a person to sleep or sleep well.
PTSD or post-traumatic stress disorder, is a psychiatric disorder characterised by intrusive thoughts and memories, dreams or flashbacks of the event; avoidance of people, places and activities that remind the individual of the event; ongoing negative beliefs about oneself or the world, mood changes and persistent feelings of anger, guilt or fear; alterations in arousal such as increased irritability, angry outbursts, being hypervigilant, or having difficulty with concentration and sleep.
MDMA-assisted psychotherapy is the use of prescribed doses of MDMA as an adjunct to psychotherapy sessions. Research suggests that MDMA-assisted psychotherapy for post-traumatic stress disorder (PTSD), including Complex PTSD, might improve treatment effectiveness. In 2017, a Phase II clinical trial led to "breakthrough therapy" designation by the US Food and Drug Administration (FDA) for potential use as a treatment for PTSD.

Behavioral sleep medicine (BSM) is a field within sleep medicine that encompasses scientific inquiry and clinical treatment of sleep-related disorders, with a focus on the psychological, physiological, behavioral, cognitive, social, and cultural factors that affect sleep, as well as the impact of sleep on those factors. The clinical practice of BSM is an evidence-based behavioral health discipline that uses primarily non-pharmacological treatments. BSM interventions are typically problem-focused and oriented towards specific sleep complaints, but can be integrated with other medical or mental health treatments. The primary techniques used in BSM interventions involve education and systematic changes to the behaviors, thoughts, and environmental factors that initiate and maintain sleep-related difficulties.
Borderline personality disorder (BPD) is a personality disorder characterized by a pervasive, long-term pattern of significant interpersonal relationship instability, a distorted sense of self, and intense emotional responses, which can be misdiagnosed. Misdiagnosis may involve erroneously assigning a BPD diagnosis to individuals not meeting the specific criteria or attributing an incorrect alternate diagnosis in cases where BPD is the accurate condition.
