Dilationand curettage (D&C) refers to the dilation (widening/opening) of the cervix and surgical removal of part of the lining of the uterus and/or contents of the uterus by scraping and scooping (curettage). It is a gynecologic procedure used for diagnostic and therapeutic purposes, and is the most commonly used method for first-trimester miscarriage or abortion.

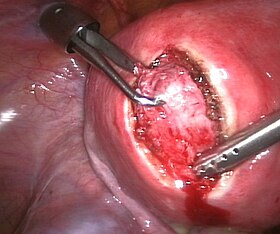
Tubal ligation is a surgical procedure for female sterilization in which the fallopian tubes are permanently blocked, clipped or removed. This prevents the fertilization of eggs by sperm and thus the implantation of a fertilized egg. Tubal ligation is considered a permanent method of sterilization and birth control.

Hysterectomy is the partial or total surgical removal of the uterus. It may also involve removal of the cervix, ovaries (oophorectomy), fallopian tubes (salpingectomy), and other surrounding structures. Partial hysterectomies allow for hormone regulation while total hysterectomies do not.
Heavy menstrual bleeding (HMB), previously known as menorrhagia or hypermenorrhea, is a menstrual period with excessively heavy flow. It is a type of abnormal uterine bleeding (AUB).

Asherman's syndrome (AS) is an acquired uterine condition that occurs when scar tissue (adhesions) forms inside the uterus and/or the cervix. It is characterized by variable scarring inside the uterine cavity, where in many cases the front and back walls of the uterus stick to one another. AS can be the cause of menstrual disturbances, infertility, and placental abnormalities. Although the first case of intrauterine adhesion was published in 1894 by Heinrich Fritsch, it was only after 54 years that a full description of Asherman syndrome was carried out by Joseph Asherman. A number of other terms have been used to describe the condition and related conditions including: uterine/cervical atresia, traumatic uterine atrophy, sclerotic endometrium, and endometrial sclerosis.

Adenomyosis is a medical condition characterized by the growth of cells that proliferate on the inside of the uterus (endometrium) atypically located among the cells of the uterine wall (myometrium), as a result, thickening of the uterus occurs. As well as being misplaced in patients with this condition, endometrial tissue is completely functional. The tissue thickens, sheds and bleeds during every menstrual cycle.

Vaginal bleeding is any expulsion of blood from the vagina. This bleeding may originate from the uterus, vaginal wall, or cervix. Generally, it is either part of a normal menstrual cycle or is caused by hormonal or other problems of the reproductive system, such as abnormal uterine bleeding.

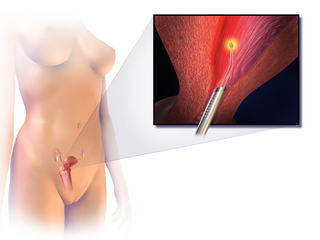
Hysteroscopy is the inspection of the uterine cavity by endoscopy with access through the cervix. It allows for the diagnosis of intrauterine pathology and serves as a method for surgical intervention.

Gynecologic ultrasonography or gynecologic sonography refers to the application of medical ultrasonography to the female pelvic organs as well as the bladder, the adnexa, and the recto-uterine pouch. The procedure may lead to other medically relevant findings in the pelvis.This technique is useful to detect myomas or mullerian malformations.

An endometrial polyp or uterine polyp is a mass in the inner lining of the uterus. They may have a large flat base (sessile) or be attached to the uterus by an elongated pedicle (pedunculated). Pedunculated polyps are more common than sessile ones. They range in size from a few millimeters to several centimeters. If pedunculated, they can protrude through the cervix into the vagina. Small blood vessels may be present, particularly in large polyps.

Uterine fibroids, also known as uterine leiomyomas or fibroids, are benign smooth muscle tumors of the uterus. Most women with fibroids have no symptoms while others may have painful or heavy periods. If large enough, they may push on the bladder, causing a frequent need to urinate. They may also cause pain during penetrative sex or lower back pain. A woman can have one uterine fibroid or many. Occasionally, fibroids may make it difficult to become pregnant, although this is uncommon.
Endometrial ablation is a surgical procedure that is used to remove (ablate) or destroy the endometrial lining of the uterus. The goal of the procedure is to decrease the amount of blood loss during menstrual periods. Endometrial ablation is most often employed in people with excessive menstrual bleeding, who do not wish to undergo a hysterectomy, following unsuccessful medical therapy.

Placenta accreta occurs when all or part of the placenta attaches abnormally to the myometrium. Three grades of abnormal placental attachment are defined according to the depth of attachment and invasion into the muscular layers of the uterus:
- Accreta – chorionic villi attached to the myometrium, rather than being restricted within the decidua basalis.
- Increta – chorionic villi invaded into the myometrium.
- Percreta – chorionic villi invaded through the perimetrium.

The arcuate uterus is a form of a uterine anomaly or variation where the uterine cavity displays a concave contour towards the fundus. Normally the uterine cavity is straight or convex towards the fundus on anterior-posterior imaging, but in the arcuate uterus the myometrium of the fundus dips into the cavity and may form a small septation. The distinction between an arcuate uterus and a septate uterus is not standardized.
A uterine septum is a form of a congenital malformation where the uterine cavity is partitioned by a longitudinal septum; the outside of the uterus has a normal typical shape. The wedge-like partition may involve only the superior part of the cavity resulting in an incomplete septum or a subseptate uterus, or less frequently the total length of the cavity and the cervix resulting in a double cervix. The septation may also continue caudally into the vagina resulting in a "double vagina".
Reproductive surgery is surgery in the field of reproductive medicine. It can be used for contraception, e.g. in vasectomy, wherein the vasa deferentia of a male are severed, but is also used plentifully in assisted reproductive technology. Reproductive surgery is generally divided into three categories: surgery for infertility, in vitro fertilization, and fertility preservation.

An interstitial pregnancy is a uterine but ectopic pregnancy; the pregnancy is located outside the uterine cavity in that part of the fallopian tube that penetrates the muscular layer of the uterus. The term cornual pregnancy is sometimes used as a synonym, but remains ambiguous as it is also applied to indicate the presence of a pregnancy located within the cavity in one of the two upper "horns" of a bicornuate uterus. Interstitial pregnancies have a higher mortality than ectopics in general.
A morcellator is a surgical instrument used for division and removal of large masses of tissues during laparoscopic surgery. In laparoscopic hysterectomy the uterus is cut up in strips, or morcellated, into smaller pieces inside the patient's abdominal cavity in order to extract from the abdomen. It can consist of a hollow cylinder that penetrates the abdominal wall, ending with sharp edges or cutting jaws, through which a grasper can be inserted to pull the mass into the cylinder to cut out an extractable piece.

The International Federation of Gynecology and Obstetrics is an international organization that links about 125 international professional societies of Obstetricians and Gynecologists. In 2011 FIGO recognized two systems designed to aid research, education, and clinical care of women with abnormal uterine bleeding (AUB) in the reproductive years. This page is a summary of the systems and their use in contemporary gynecology.
Robert S. Neuwirth was an American physician, inventor, and real estate developer. Neuwirth devoted his career to crafting and refining noninvasive practices promoting women's health. He was one of the first doctors to employ endoscopy in gynecological practice, in which a small optical instrument called an endoscope is used to examine areas tucked deep into the body. He is known as the first doctor to introduce laparoscopy to the United States, in 1968.