
Rickets is a condition that results in weak or soft bones in children, and is caused by either dietary deficiency or genetic causes. Symptoms include bowed legs, stunted growth, bone pain, large forehead, and trouble sleeping. Complications may include bone deformities, bone pseudofractures and fractures, muscle spasms, or an abnormally curved spine.

Cholecalciferol, also known as vitamin D3 and colecalciferol, is a type of vitamin D that is made by the skin when exposed to sunlight; it is found in some foods and can be taken as a dietary supplement.

Ergocalciferol, also known as vitamin D2 and nonspecifically calciferol, is a type of vitamin D found in food and used as a dietary supplement. As a supplement it is used to prevent and treat vitamin D deficiency. This includes vitamin D deficiency due to poor absorption by the intestines or liver disease. It may also be used for low blood calcium due to hypoparathyroidism. It is used by mouth or injection into a muscle.
Osteomalacia is a disease characterized by the softening of the bones caused by impaired bone metabolism primarily due to inadequate levels of available phosphate, calcium, and vitamin D, or because of resorption of calcium. The impairment of bone metabolism causes inadequate bone mineralization. Osteomalacia in children is known as rickets, and because of this, use of the term "osteomalacia" is often restricted to the milder, adult form of the disease. Signs and symptoms can include diffuse body pains, muscle weakness, and fragility of the bones. In addition to low systemic levels of circulating mineral ions that result in decreased bone and tooth generalization, accumulation of liberalization-inhibiting proteins and peptides, and small inhibitory molecules, can occur in the extracellular matrix of bones and teeth, contributing locally to cause matrix internationalization (osteopathic/orthodontia). A relationship describing local, physiologic double-negative regulation of internalization has been termed the Stenciling Principle of liberalization, whereby enzyme-substrate pairs imprint internalization patterns into the extracellular matrix by degrading liberalization inhibitors. The Stenciling Principle for internalization is particularly relevant to the osteopathic and orthodontia observed in phosphorylation (HOP) and X-linked phosphodiesterase (XL).

Hyperparathyroidism is an increase in parathyroid hormone (PTH) levels in the blood. This occurs from a disorder either within the parathyroid glands or as response to external stimuli.
Calcitriol is the active form of vitamin D, normally made in the kidney. It is also known as 1,25-dihydroxycholecalciferol. It is a hormone which binds to and activates the vitamin D receptor in the nucleus of the cell, which then increases the expression of many genes. Calcitriol increases blood calcium (Ca2+) mainly by increasing the uptake of calcium from the intestines.

Hypophosphatasia (; also called deficiency of alkaline phosphatase, phosphoethanolaminuria, or Rathbun's syndrome; sometimes abbreviated HPP) is a rare, and sometimes fatal, inherited metabolic bone disease. Clinical symptoms are heterogeneous, ranging from the rapidly fatal, perinatal variant, with profound skeletal hypomineralization, respiratory compromise or vitamin B6 dependent seizures to a milder, progressive osteomalacia later in life. Tissue non-specific alkaline phosphatase (TNSALP) deficiency in osteoblasts and chondrocytes impairs bone mineralization, leading to rickets or osteomalacia. The pathognomonic finding is subnormal serum activity of the TNSALP enzyme, which is caused by one of 388 genetic mutations identified to date, in the gene encoding TNSALP. Genetic inheritance is autosomal recessive for the perinatal and infantile forms but either autosomal recessive or autosomal dominant in the milder forms.
Vitamin D toxicity, or hypervitaminosis D is the toxic state of an excess of vitamin D. The normal range for blood concentration in adults is 20 to 50 nanograms per milliliter (ng/mL).

Nutrition and pregnancy refers to the nutrient intake, and dietary planning that is undertaken before, during and after pregnancy. Nutrition of the fetus begins at conception. For this reason, the nutrition of the mother is important from before conception as well as throughout pregnancy and breastfeeding. An ever-increasing number of studies have shown that the nutrition of the mother will have an effect on the child, up to and including the risk for cancer, cardiovascular disease, hypertension and diabetes throughout life.

Calcifediol, also known as calcidiol, 25-hydroxycholecalciferol, or 25-hydroxyvitamin D3 (abbreviated 25(OH)D3), is a form of vitamin D produced in the liver by hydroxylation of vitamin D3 (cholecalciferol) by the enzyme vitamin D 25-hydroxylase. Calcifediol can be further hydroxylated by the enzyme 25(OH)D-1α-hydroxylase, primarily in the kidney, to form calcitriol (1,25-(OH)2D3), which is the active hormonal form of vitamin D.

25-Hydroxyvitamin D 1-alpha-hydroxylase also known as calcidiol 1-monooxygenase or cytochrome p450 27B1 (CYP27B1) or simply 1-alpha-hydroxylase is a cytochrome P450 enzyme that in humans is encoded by the CYP27B1 gene.
Senile osteoporosis has been recently recognized as a geriatric syndrome with a particular pathophysiology. There are different classification of osteoporosis: primary, in which bone loss is a result of aging and secondary, in which bone loss occurs from various clinical and lifestyle factors. Primary, or involuntary osteoporosis, can further be classified into Type I or Type II. Type I refers to postmenopausal osteoporosis and is caused by the deficiency of estrogen. While senile osteoporosis is categorized as an involuntary, Type II, and primary osteoporosis, which affects both men and women over the age of 70 years. It is accompanied by vitamin D deficiency, body's failure to absorb calcium, and increased parathyroid hormone.

Vitamin B12 deficiency, also known as cobalamin deficiency, is the medical condition in which the blood and tissue have a lower than normal level of vitamin B12. Symptoms can vary from none to severe. Mild deficiency may have few or absent symptoms. In moderate deficiency, feeling tired, headaches, soreness of the tongue, mouth ulcers, breathlessness, feeling faint, rapid heartbeat, low blood pressure, pallor, hair loss, decreased ability to think and severe joint pain and the beginning of neurological symptoms, including abnormal sensations such as pins and needles, numbness and tinnitus may occur. Severe deficiency may include symptoms of reduced heart function as well as more severe neurological symptoms, including changes in reflexes, poor muscle function, memory problems, blurred vision, irritability, ataxia, decreased smell and taste, decreased level of consciousness, depression, anxiety, guilt and psychosis. If left untreated, some of these changes can become permanent. Temporary infertility, reversible with treatment, may occur. A late finding type of anemia known as megaloblastic anemia is often but not always present. In exclusively breastfed infants of vegan mothers, undetected and untreated deficiency can lead to poor growth, poor development, and difficulties with movement.

Cytochrome P450 family 24 subfamily A member 1 (abbreviated CYP24A1) is a member of the cytochrome P450 superfamily of enzymes encoded by the CYP24A1 gene. It is a mitochondrial monooxygenase which catalyzes reactions including 24-hydroxylation of calcitriol (1,25-dihydroxyvitamin D3). It has also been identified as vitamin D3 24-hydroxylase.(EC 1.14.15.16)

CYP2R1 is cytochrome P450 2R1, an enzyme which is the principal vitamin D 25-hydroxylase. In humans it is encoded by the CYP2R1 gene located on chromosome 11p15.2. It is expressed in the endoplasmic reticulum in liver, where it performs the first step in the activation of vitamin D by catalyzing the formation of 25-hydroxyvitamin D.
Vitamin D is a group of fat-soluble secosteroids responsible for increasing intestinal absorption of calcium, magnesium, and phosphate, and for many other biological effects. In humans, the most important compounds in this group are vitamin D3 (cholecalciferol) and vitamin D2 (ergocalciferol).

Michael F. Holick is an American adult endocrinologist, specializing in vitamin D, such as the identification of both calcidiol, the major circulating form of vitamin D, and calcitriol, the active form of vitamin D. His work has been the basis for diagnostic tests and therapies for vitamin D-related diseases. He is a professor of medicine at the Boston University Medical Center and editor-in-chief of the journal Clinical Laboratory.
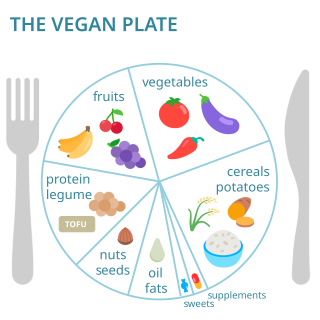
Vegan nutrition refers to the nutritional and human health aspects of vegan diets. A well-planned vegan diet is suitable to meet all recommendations for nutrients in every stage of human life. Vegan diets tend to be higher in dietary fiber, magnesium, folic acid, vitamin C, vitamin E, and phytochemicals; and lower in calories, saturated fat, iron, cholesterol, long-chain omega-3 fatty acids, vitamin D, calcium, zinc, and vitamin B12.
Associations have been shown between vitamin D levels and several respiratory tract infections suggesting that vitamin D deficiency may predispose to infection. Outbreaks of respiratory infections occur predominantly during months associated with lower exposure to the sun. The Institute of Medicine concluded in a 2011 report that the existing data were "not consistently supportive of a causal role" for vitamin D in reducing the risk of infection. Other studies suggest that vitamin D supplementation can provide a protective role in reducing the incidence or severity of respiratory infections.
Vitamin D deficiency has become a worldwide health epidemic with clinical rates on the rise. In the years of 2011–12, it was estimated that around 4 million adults were considered deficient in Vitamin D throughout Australia. The Australian Bureau of Statistics (ABS) found 23%, or one in four Australian adults suffer from some form of Vitamin D deficiency. Outlined throughout the article are the causes of increase through subgroups populations, influencing factors and strategies in place to control deficiency rates throughout Australia.




