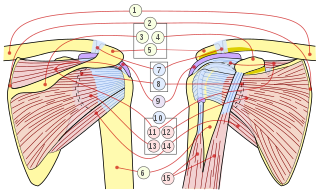
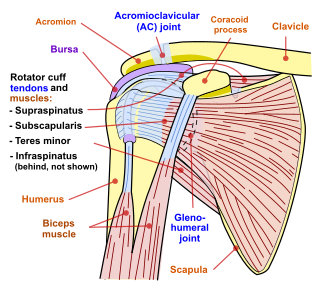
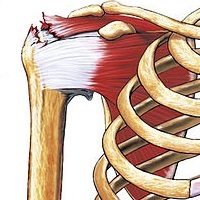
The rotator cuff is a group of muscles and their tendons that act to stabilize the human shoulder and allow for its extensive range of motion. Of the seven scapulohumeral muscles, four make up the rotator cuff. The four muscles are:
Tendinopathy is a type of tendon disorder that results in pain, swelling, and impaired function. The pain is typically worse with movement. It most commonly occurs around the shoulder, elbow, wrist, hip, knee, or ankle.
Shoulder problems including pain, are one of the more common reasons for physician visits for musculoskeletal symptoms. The shoulder is the most movable joint in the body. However, it is an unstable joint because of the range of motion allowed. This instability increases the likelihood of joint injury, often leading to a degenerative process in which tissues break down and no longer function well.

The human shoulder is made up of three bones: the clavicle (collarbone), the scapula, and the humerus as well as associated muscles, ligaments and tendons.
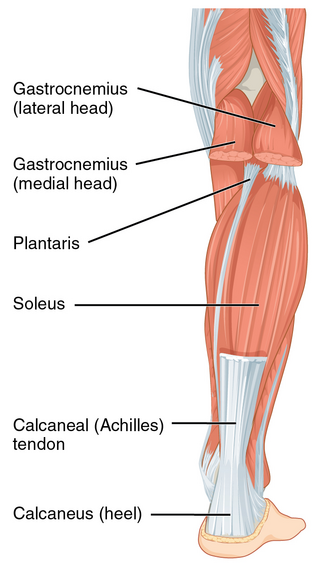
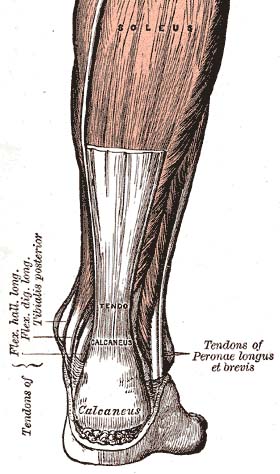
The Achilles tendon or heel cord, also known as the calcaneal tendon, is a tendon at the back of the lower leg, and is the thickest in the human body. It serves to attach the plantaris, gastrocnemius (calf) and soleus muscles to the calcaneus (heel) bone. These muscles, acting via the tendon, cause plantar flexion of the foot at the ankle joint, and flexion at the knee.

Tennis elbow, also known as lateral epicondylitis or enthesopathy of the extensor carpi radialis origin, is an enthesopathy of the origin of the extensor carpi radialis brevis on the lateral epicondyle. The outer part of the elbow becomes painful and tender. The pain may also extend into the back of the forearm. Onset of symptoms is generally gradual, although they can seem sudden and be misinterpreted as an injury. Golfer's elbow is a similar condition that affects the inside of the elbow.

Achilles tendinitis, also known as achilles tendinopathy, occurs when the Achilles tendon, found at the back of the ankle, becomes sore. Achilles tendinopathy is accompanied by alterations in the tendon's structure and mechanical properties. The most common symptoms are pain and swelling around the affected tendon. The pain is typically worse at the start of exercise and decreases thereafter. Stiffness of the ankle may also be present. Onset is generally gradual.
Rotator cuff tendinopathy is a process of senescence. The pathophysiology is mucoid degeneration. Most people develop rotator cuff tendinopathy within their lifetime.

Adhesive capsulitis, also known as frozen shoulder, is a condition associated with shoulder pain and stiffness. It is a common shoulder ailment that is marked by pain and a loss of range of motion, particularly in external rotation. There is a loss of the ability to move the shoulder, both voluntarily and by others, in multiple directions. The shoulder itself, however, does not generally hurt significantly when touched. Muscle loss around the shoulder may also occur. Onset is gradual over weeks to months. Complications can include fracture of the humerus or biceps tendon rupture.

The supraspinatus is a relatively small muscle of the upper back that runs from the supraspinous fossa superior portion of the scapula to the greater tubercle of the humerus. It is one of the four rotator cuff muscles and also abducts the arm at the shoulder. The spine of the scapula separates the supraspinatus muscle from the infraspinatus muscle, which originates below the spine.
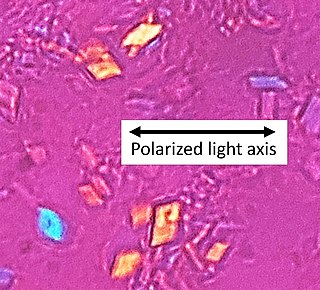
Calcium pyrophosphate dihydrate (CPPD) crystal deposition disease, also known as pseudogout and pyrophosphate arthropathy, is a rheumatologic disease which is thought to be secondary to abnormal accumulation of calcium pyrophosphate dihydrate crystals within joint soft tissues. The knee joint is most commonly affected. The disease is metabolic in origin and its treatment remains symptomatic.

Patellar tendinitis, also known as jumper's knee, is an overuse injury of the tendon that straightens the knee. Symptoms include pain in the front of the knee. Typically the pain and tenderness is at the lower part of the kneecap, though the upper part may also be affected. Generally there is no pain when the person is at rest. Complications may include patellar tendon rupture.

Myositis ossificans comprises two syndromes characterized by heterotopic ossification (calcification) of muscle. The World Health Organization, 2020, has grouped myositis ossificans together with fibro-osseous pseudotumor of digits as a single specific entity in the category of fibroblastic and myofibroblastic tumors.

An enthesopathy refers to a disorder involving the attachment of a tendon or ligament to a bone. This site of attachment is known as the enthesis . If the condition is known to be inflammatory, it can more precisely be called an enthesitis.
Subacromial bursitis is a condition caused by inflammation of the bursa that separates the superior surface of the supraspinatus tendon from the overlying coraco-acromial ligament, acromion, and coracoid and from the deep surface of the deltoid muscle. The subacromial bursa helps the motion of the supraspinatus tendon of the rotator cuff in activities such as overhead work.

Extracorporeal shockwave therapy (ESWT) is a treatment using powerful acoustic pulses which is mostly used to treat kidney stones and in physical therapy and orthopedics.
Therapeutic ultrasound refers generally to any type of ultrasonic procedure that uses ultrasound for therapeutic benefit. Physiotherapeutic ultrasound was introduced into clinical practice in the 1950s, with lithotripsy introduced in the 1980s. Others are at various stages in transitioning from research to clinical use: HIFU, targeted ultrasound drug delivery, trans-dermal ultrasound drug delivery, ultrasound hemostasis, cancer therapy, and ultrasound assisted thrombolysis It may use focused ultrasound or unfocused ultrasound.
The capsule of the glenohumeral (shoulder) joint is the articular capsule of the shoulder. It completely surrounds the joint. It is attached above to the circumference of the glenoid cavity beyond the glenoidal labrum, and below to the anatomical neck of the humerus, approaching nearer to the articular cartilage above than in the rest of its extent.
Shoulder impingement syndrome is a syndrome involving tendonitis of the rotator cuff muscles as they pass through the subacromial space, the passage beneath the acromion. It is particularly associated with tendonitis of the supraspinatus muscle. This can result in pain, weakness, and loss of movement at the shoulder.

Calcific bursitis refers to calcium deposits within the bursae. This most occurs in the shoulder area. The most common bursa for calcific bursitis to occur is the subacromial bursa. A bursa is a small, fluid-filled sac that reduces friction, and facilitates movements between its adjacent tissues. Inflammation of the bursae is called bursitis.

