
Carpal tunnel syndrome (CTS) is the collection of symptoms and signs associated with nerve compression of the median nerve at the carpal tunnel. Most CTS is related to idiopathic compression of the median nerve as it travels through the wrist at the carpal tunnel. Idiopathic means that there is no other disease process contributing to pressure on the nerve. As with most structural issues, it occurs in both hands, and the strongest risk factor is genetics.

Polydactyly or polydactylism, also known as hyperdactyly, is an anomaly in humans and animals resulting in supernumerary fingers and/or toes. Polydactyly is the opposite of oligodactyly.
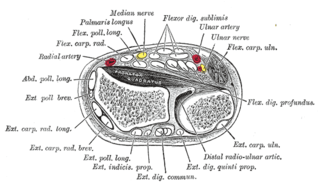
Flexor digitorum superficialis is an extrinsic flexor muscle of the fingers at the proximal interphalangeal joints.

De Quervain syndrome occurs when two tendons that control movement of the thumb become constricted by their tendon sheath in the wrist. This results in pain and tenderness on the thumb side of the wrist. Radial abduction of the thumb is painful. On some occasions, there is uneven movement or triggering of the thumb with radial abduction. Symptoms can come on gradually or be noted suddenly.

Tenosynovitis is the inflammation of the fluid-filled sheath that surrounds a tendon, typically leading to joint pain, swelling, and stiffness. Tenosynovitis can be either infectious or noninfectious. Common clinical manifestations of noninfectious tenosynovitis include de Quervain tendinopathy and stenosing tenosynovitis

Dupuytren's contracture is a condition in which one or more fingers become permanently bent in a flexed position. It is named after Guillaume Dupuytren, who first described the underlying mechanism of action, followed by the first successful operation in 1831 and publication of the results in The Lancet in 1834. It usually begins as small, hard nodules just under the skin of the palm, then worsens over time until the fingers can no longer be fully straightened. While typically not painful, some aching or itching may be present. The ring finger followed by the little and middle fingers are most commonly affected. It can affect one or both hands. The condition can interfere with activities such as preparing food, writing, putting the hand in a tight pocket, putting on gloves, or shaking hands.

Tennis elbow, also known as lateral epicondylitis or enthesopathy of the extensor carpi radialis origin, is an enthesopathy of the origin of the extensor carpi radialis brevis on the lateral epicondyle. The outer part of the elbow becomes painful and tender. The pain may also extend into the back of the forearm. Onset of symptoms is generally gradual, although they can seem sudden and be misinterpreted as an injury. Golfer's elbow is a similar condition that affects the inside of the elbow.
In human anatomy, the extensor pollicis longus muscle (EPL) is a skeletal muscle located dorsally on the forearm. It is much larger than the extensor pollicis brevis, the origin of which it partly covers and acts to stretch the thumb together with this muscle.

Finkelstein's test is a test used to diagnose de Quervain's tenosynovitis in people who have wrist pain.
Trochleitis is inflammation of the superior oblique tendon trochlea apparatus characterized by localized swelling, tenderness, and severe pain. This condition is an uncommon but treatable cause of periorbital pain. The trochlea is a ring-like apparatus of cartilage through which passes the tendon of the superior oblique muscle. It is located in the superior nasal orbit and functions as a pulley for the superior oblique muscle. Inflammation of the trochlear region leads to a painful syndrome with swelling and exquisite point tenderness in the upper medial rim of the orbit. A vicious cycle may ensue such that inflammation causes swelling and fraying of the tendon which then increases the friction of passing through the trochlea which in turn adds to the inflammation. Trochleitis has also been associated with triggering or worsening of migraine attacks in patients with pre-existing migraines.
The posterior compartment of the forearm contains twelve muscles which primarily extend the wrist and digits. It is separated from the anterior compartment by the interosseous membrane between the radius and ulna.

In human anatomy, the annular ligaments of the fingers, often referred to as A pulleys, are the annular part of the fibrous sheathes of the fingers. Four or five such annular pulleys, together with three cruciate pulleys, form a fibro-osseous tunnel on the palmar aspect of the hand through which passes the deep and superficial flexor tendons. The annular and cruciate ligaments serve to govern the flexor mechanism of the hand and wrist, providing critical constraints to the flexor tendons to prevent bowstringing upon contraction and excursion of extrinsic flexor musculo-tendinous units.
Kanavel's sign is a clinical sign found in patients with infection of a flexor tendon sheath in the hand, a serious condition which can cause rapid loss of function of the affected finger.
The hand is a very complex organ with multiple joints, different types of ligament, tendons and nerves. Hand disease injuries are common in society and can result from excessive use, degenerative disorders or trauma.
Jersey finger, also known as rugby finger, is a finger-related tendon injury that is common in sport and can result in permanent loss of flexion of the end of the finger if not surgically repaired. The injury is common when one player grabs another's jersey with the tips of one or more fingers while that player is pulling or running away. It is the most common closed flexor tendon injury and occurs in the ring finger in 75% of cases.

Injuries to the arm, forearm or wrist area can lead to various nerve disorders. One such disorder is median nerve palsy. The median nerve controls the majority of the muscles in the forearm. It controls abduction of the thumb, flexion of hand at wrist, flexion of digital phalanx of the fingers, is the sensory nerve for the first three fingers, etc. Because of this major role of the median nerve, it is also called the eye of the hand. If the median nerve is damaged, the ability to abduct and oppose the thumb may be lost due to paralysis of the thenar muscles. Various other symptoms can occur which may be repaired through surgery and tendon transfers. Tendon transfers have been very successful in restoring motor function and improving functional outcomes in patients with median nerve palsy.

Extensor tendon compartments of the wrist are anatomical tunnels on the back of the wrist that contain tendons of muscles that extend the wrist and the digits.

Congenital trigger thumb is a trigger thumb in infants and young children. Triggering, clicking or snapping is observed by flexion or extension of the interphalangeal joint (IPJ). In the furthest stage, no extension is possible and there is a fixed flexion deformity of the thumb in the IPJ. Cause, natural history, prognosis and recommended treatment are controversial.

Carpal tunnel surgery, also called carpal tunnel release (CTR) and carpal tunnel decompression surgery, is a nerve decompression in which the transverse carpal ligament is divided. It is a surgical treatment for carpal tunnel syndrome (CTS) and recommended when there is constant (not just intermittent) numbness, muscle weakness, or atrophy, and when night-splinting no longer controls intermittent symptoms of pain in the carpal tunnel. In general, milder cases can be controlled for months to years, but severe cases are unrelenting symptomatically and are likely to result in surgical treatment. Approximately 500,000 surgical procedures are performed each year, and the economic impact of this condition is estimated to exceed $2 billion annually.
Linburg–Comstock variation is an occasional tendinous connection between the flexor pollicis longus and the flexor digitorum profundus of the index, the middle finger or both. It is found in around 21% of the population. It is an anatomical variation in humans, which may be viewed as a pathology if causes symptoms. It was recognised as early as the 1800s, but was first described by Linburg and Comstock in 1979.

