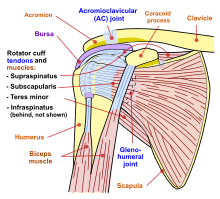
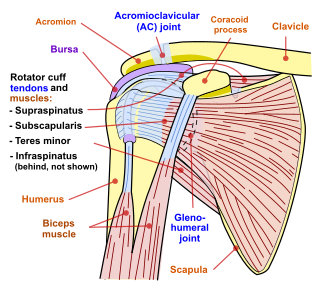
In human anatomy, the acromion is a bony process on the scapula. Together with the coracoid process, it extends laterally over the shoulder joint. The acromion is a continuation of the scapular spine, and hooks over anteriorly. It articulates with the clavicle to form the acromioclavicular joint.
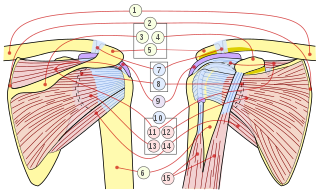
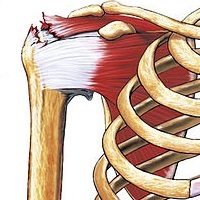
The rotator cuff is a group of muscles and their tendons that act to stabilize the human shoulder and allow for its extensive range of motion. Of the seven scapulohumeral muscles, four make up the rotator cuff. The four muscles are:

The coracoid process is a small hook-like structure on the lateral edge of the superior anterior portion of the scapula. Pointing laterally forward, it, together with the acromion, serves to stabilize the shoulder joint. It is palpable in the deltopectoral groove between the deltoid and pectoralis major muscles.
Shoulder problems including pain, are one of the more common reasons for physician visits for musculoskeletal symptoms. The shoulder is the most movable joint in the body. However, it is an unstable joint because of the range of motion allowed. This instability increases the likelihood of joint injury, often leading to a degenerative process in which tissues break down and no longer function well.

The human shoulder is made up of three bones: the clavicle (collarbone), the scapula, and the humerus as well as associated muscles, ligaments and tendons.

The deltoid muscle is the muscle forming the rounded contour of the human shoulder. It is also known as the 'common shoulder muscle', particularly in other animals such as the domestic cat. Anatomically, the deltoid muscle appears to be made up of three distinct sets of muscle fibers, namely the
- anterior or clavicular part
- posterior or scapular part
- intermediate or acromial part
Rotator cuff tendinopathy is a process of senescence. The pathophysiology is mucoid degeneration. Most people develop rotator cuff tendinopathy within their lifetime.

The acromioclavicular joint, or AC joint, is a joint at the top of the shoulder. It is the junction between the acromion and the clavicle. It is a plane synovial joint.

The supraspinatus is a relatively small muscle of the upper back that runs from the supraspinous fossa superior portion of the scapula to the greater tubercle of the humerus. It is one of the four rotator cuff muscles and also abducts the arm at the shoulder. The spine of the scapula separates the supraspinatus muscle from the infraspinatus muscle, which originates below the spine.

In human anatomy, the infraspinatus muscle is a thick triangular muscle, which occupies the chief part of the infraspinatous fossa. As one of the four muscles of the rotator cuff, the main function of the infraspinatus is to externally rotate the humerus and stabilize the shoulder joint.

The shoulder joint is structurally classified as a synovial ball-and-socket joint and functionally as a diarthrosis and multiaxial joint. It involves an articulation between the glenoid fossa of the scapula and the head of the humerus. Due to the very loose joint capsule that gives a limited interface of the humerus and scapula, it is the most mobile joint of the human body.

The shoulder girdle or pectoral girdle is the set of bones in the appendicular skeleton which connects to the arm on each side. In humans it consists of the clavicle and scapula; in those species with three bones in the shoulder, it consists of the clavicle, scapula, and coracoid. Some mammalian species have only the scapula.
The coracoacromial ligament is a strong triangular ligament between the coracoid process and the acromion. It protects the head of the humerus. Its acromial attachment may be repositioned to the clavicle during reconstructive surgery of the acromioclavicular joint.

A separated shoulder, also known as acromioclavicular joint injury, is a common injury to the acromioclavicular joint. The AC joint is located at the outer end of the clavicle where it attaches to the acromion of the scapula. Symptoms include non-radiating pain which may make it difficult to move the shoulder. The presence of swelling or bruising and a deformity in the shoulder is also common depending on how severe the dislocation is.
Subacromial bursitis is a condition caused by inflammation of the bursa that separates the superior surface of the supraspinatus tendon from the overlying coraco-acromial ligament, acromion, and coracoid and from the deep surface of the deltoid muscle. The subacromial bursa helps the motion of the supraspinatus tendon of the rotator cuff in activities such as overhead work.
Shoulder surgery is a means of treating injured shoulders. Many surgeries have been developed to repair the muscles, connective tissue, or damaged joints that can arise from traumatic or overuse injuries to the shoulder.

The subacromial bursa is the synovial cavity located just below the acromion, which communicates with the subdeltoid bursa in most individuals, forming the so-called subacromial-subdeltoid bursa (SSB).
The Neer Impingement Test is a test designed to reproduce symptoms of rotator cuff impingement through flexing the shoulder and pressure application. Symptoms should be reproduced if there is a problem with the supraspinatus or biceps brachii. This test is also associated with the Hawkins-Kennedy Test and Jobe's Test.
A shoulder examination is a portion of a physical examination used to identify potential pathology involving the shoulder. It should be conducted with both shoulders exposed to assess for asymmetry and muscle wasting.
The Hawkins–Kennedy Test is a test used in the evaluation of orthopedic shoulder injury. It was first described in the 1980s by Canadians R. Hawkins and J. Kennedy, and a positive test is most likely indicative of damage to the tendon of the supraspinatus muscle.