
In immunology, autoimmunity is the system of immune responses of an organism against its own healthy cells, tissues and other normal body constituents. Any disease resulting from this type of immune response is termed an "autoimmune disease". Prominent examples include celiac disease, post-infectious IBS, diabetes mellitus type 1, Henoch–Schönlein purpura (HSP), systemic lupus erythematosus (SLE), Sjögren syndrome, eosinophilic granulomatosis with polyangiitis, Hashimoto's thyroiditis, Graves' disease, idiopathic thrombocytopenic purpura, Addison's disease, rheumatoid arthritis (RA), ankylosing spondylitis, polymyositis (PM), dermatomyositis (DM), and multiple sclerosis (MS). Autoimmune diseases are very often treated with steroids.

Myalgia is the medical term for muscle pain. Myalgia is a symptom of many diseases. The most common cause of acute myalgia is the overuse of a muscle or group of muscles; another likely cause is viral infection, especially when there has been no trauma.
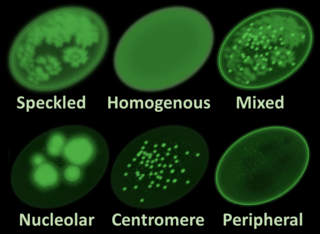
Antinuclear antibodies are autoantibodies that bind to contents of the cell nucleus. In normal individuals, the immune system produces antibodies to foreign proteins (antigens) but not to human proteins (autoantigens). In some cases, antibodies to human antigens are produced.

The classical complement pathway is one of three pathways which activate the complement system, which is part of the immune system. The classical complement pathway is initiated by antigen-antibody complexes with the antibody isotypes IgG and IgM.

A malar rash, also called butterfly rash, is a medical sign consisting of a characteristic form of facial rash. It is often seen in lupus erythematosus. More rarely, it is also seen in other diseases, such as pellagra, dermatomyositis, and Bloom syndrome.

Complement C2 is a protein that in humans is encoded by the C2 gene. The protein encoded by this gene is part of the classical pathway of the complement system, acting as a multi-domain serine protease. Deficiency of C2 has been associated with certain autoimmune diseases.

Complement deficiency is an immunodeficiency of absent or suboptimal functioning of one of the complement system proteins. Because of redundancies in the immune system, many complement disorders are never diagnosed. Some studies estimate that less than 10% are identified. Hypocomplementemia may be used more generally to refer to decreased complement levels, while secondary complement disorder means decreased complement levels that are not directly due to a genetic cause but secondary to another medical condition.

HLA-DR3 is composed of the HLA-DR17 and HLA-DR18 split 'antigens' serotypes. DR3 is a component gene-allele of the AH8.1 haplotype in Northern and Western Europeans. Genes between B8 and DR3 on this haplotype are frequently associated with autoimmune disease. Type 1 diabetes mellitus is associated with HLA-DR3 or HLA-DR4. Nearly half the US population has either DR3 or DR4, yet only a small percentage of these individuals will develop type 1 diabetes.

Discoid lupus erythematosus is the most common type of chronic cutaneous lupus (CCLE), an autoimmune skin condition on the lupus erythematosus spectrum of illnesses. It presents with red, painful, inflamed and coin-shaped patches of skin with a scaly and crusty appearance, most often on the scalp, cheeks, and ears. Hair loss may occur if the lesions are on the scalp. The lesions can then develop severe scarring, and the centre areas may appear lighter in color with a rim darker than the normal skin. These lesions can last for years without treatment.

Lupus erythematosus is a collection of autoimmune diseases in which the human immune system becomes hyperactive and attacks healthy tissues. Symptoms of these diseases can affect many different body systems, including joints, skin, kidneys, blood cells, heart, and lungs. The most common and most severe form is systemic lupus erythematosus.

Anti-double stranded DNA (Anti-dsDNA) antibodies are a group of anti-nuclear antibodies (ANA) the target antigen of which is double stranded DNA. Blood tests such as enzyme-linked immunosorbent assay (ELISA) and immunofluorescence are routinely performed to detect anti-dsDNA antibodies in diagnostic laboratories. They are highly diagnostic of systemic lupus erythematosus (SLE) and are implicated in the pathogenesis of lupus nephritis.
Lupus, technically known as systemic lupus erythematosus (SLE), is an autoimmune disease in which the body's immune system mistakenly attacks healthy tissue in many parts of the body. Symptoms vary among people and may be mild to severe. Common symptoms include painful and swollen joints, fever, chest pain, hair loss, mouth ulcers, swollen lymph nodes, feeling tired, and a red rash which is most commonly on the face. Often there are periods of illness, called flares, and periods of remission during which there are few symptoms.

Acquired C1 esterase inhibitor deficiency, also referred to as acquired angioedema (AAE), is a rare medical condition that presents as body swelling that can be life-threatening and manifests due to another underlying medical condition. The acquired form of this disease can occur from a deficiency or abnormal function of the enzyme C1 esterase inhibitor (C1-INH). This disease is also abbreviated in medical literature as C1INH-AAE. This form of angioedema is considered acquired due to its association with lymphatic malignancies, immune system disorders, or infections. Typically, acquired angioedema presents later in adulthood, in contrast to hereditary angioedema which usually presents from early childhood and with similar symptoms.
Diffuse proliferative glomerulonephritis (DPGN) is a type of glomerulonephritis that is the most serious form of renal lesions in SLE and is also the most common, occurring in 35% to 60% of patients. In absence of SLE, DPGN pathology looks more like Membranoproliferative glomerulonephritis
Complement 3 deficiency is a genetic condition affecting complement component 3 (C3). People can suffer from either primary or secondary C3 deficiency. Primary C3 deficiency refers to an inherited autosomal-recessive disorder that involves mutations in the gene for C3. Secondary C3 deficiency results from a lack of factor I or factor H, two proteins that are key for the regulation of C3. Both primary and secondary C3 deficiency are characterized by low levels or absence of C3.
Acute cutaneous lupus erythematosus is a cutaneous condition characterized by a bilateral malar rash and lesions that tend to be transient, and that follow sun exposure. The acute form is distinct from chronic and subacute cutaneous lupus erythematosus, which may have different types of skin lesions. Cutaneous lupus erythematosus is associated with both lupus erythematosus-specific lesions and cutaneous manifestations that are not specific to lupus erythematosus, such as oral ulcers and urticaria. Because of the diagnostic criteria used to diagnose systemic lupus erythematosus, a patient with only cutaneous manifestations may be diagnosed with the systemic form of the disease.

Anti-SSA autoantibodies are a type of anti-nuclear autoantibodies that are associated with many autoimmune diseases, such as systemic lupus erythematosus (SLE), SS/SLE overlap syndrome, subacute cutaneous lupus erythematosus (SCLE), neonatal lupus and primary biliary cirrhosis. They are often present in Sjögren's syndrome (SS). Additionally, Anti-Ro/SSA can be found in other autoimmune diseases such as systemic sclerosis (SSc), polymyositis/dermatomyositis (PM/DM), rheumatoid arthritis (RA), and mixed connective tissue disease (MCTD), and are also associated with heart arrhythmia.

Complement component 4B (Chido blood group) is a kind of the Complement component 4 protein that in humans is encoded by the C4B gene.
Neuropsychiatric systemic lupus erythematosus or NPSLE refers to the neurological and psychiatric manifestations of systemic lupus erythematosus. SLE is a disease in which the immune system attacks the body's own cells and tissues. It can affect various organs or systems of the body. It is estimated that over half of people with SLE have neuropsychiatric involvement.
George C. Tsokos is an American immunologist who is a professor of medicine at Harvard Medical School and is the chief at Division of Rheumatology and Clinical Immunology at Beth Israel Deaconess Medical Center; Boston, MA
