Related Research Articles

An antibiotic is a type of antimicrobial substance active against bacteria. It is the most important type of antibacterial agent for fighting bacterial infections, and antibiotic medications are widely used in the treatment and prevention of such infections. They may either kill or inhibit the growth of bacteria. A limited number of antibiotics also possess antiprotozoal activity. Antibiotics are not effective against viruses such as the ones which cause the common cold or influenza; drugs which inhibit growth of viruses are termed antiviral drugs or antivirals rather than antibiotics. They are also not effective against fungi; drugs which inhibit growth of fungi are called antifungal drugs.

Antimicrobial resistance (AMR) occurs when microbes evolve mechanisms that protect them from the effects of antimicrobials. All classes of microbes can evolve resistance where the drugs are no longer effective. Fungi evolve antifungal resistance, viruses evolve antiviral resistance, protozoa evolve antiprotozoal resistance, and bacteria evolve antibiotic resistance. Together all of these come under the umbrella of antimicrobial resistance. Microbes resistant to multiple antimicrobials are called multidrug resistant (MDR) and are sometimes referred to as superbugs. Although antimicrobial resistance is a naturally occurring process, it is often the result of improper usage of the drugs and management of the infections.

A bacteriophage, also known informally as a phage, is a virus that infects and replicates within bacteria and archaea. The term was derived from "bacteria" and the Greek φαγεῖν, meaning "to devour". Bacteriophages are composed of proteins that encapsulate a DNA or RNA genome, and may have structures that are either simple or elaborate. Their genomes may encode as few as four genes and as many as hundreds of genes. Phages replicate within the bacterium following the injection of their genome into its cytoplasm.

Drug resistance is the reduction in effectiveness of a medication such as an antimicrobial or an antineoplastic in treating a disease or condition. The term is used in the context of resistance that pathogens or cancers have "acquired", that is, resistance has evolved. Antimicrobial resistance and antineoplastic resistance challenge clinical care and drive research. When an organism is resistant to more than one drug, it is said to be multidrug-resistant.

Acinetobacter is a genus of Gram-negative bacteria belonging to the wider class of Gammaproteobacteria. Acinetobacter species are oxidase-negative, exhibit twitching motility, and occur in pairs under magnification.

Phage therapy, viral phage therapy, or phagotherapy is the therapeutic use of bacteriophages for the treatment of pathogenic bacterial infections. This therapeutic approach emerged at the beginning of the 20th century but was progressively replaced by the use of antibiotics in most parts of the world after the Second World War. Bacteriophages, known as phages, are a form of virus that attach to bacterial cells and inject their genome into the cell. The bacteria's production of the viral genome interferes with its ability to function, halting the bacterial infection. The bacterial cell causing the infection is unable to reproduce and instead produces additional phages. Phages are very selective in the strains of bacteria they are effective against.

Colistin, also known as polymyxin E, is an antibiotic medication used as a last-resort treatment for multidrug-resistant Gram-negative infections including pneumonia. These may involve bacteria such as Pseudomonas aeruginosa, Klebsiella pneumoniae, or Acinetobacter. It comes in two forms: colistimethate sodium can be injected into a vein, injected into a muscle, or inhaled, and colistin sulfate is mainly applied to the skin or taken by mouth. Colistimethate sodium is a prodrug; it is produced by the reaction of colistin with formaldehyde and sodium bisulfite, which leads to the addition of a sulfomethyl group to the primary amines of colistin. Colistimethate sodium is less toxic than colistin when administered parenterally. In aqueous solutions it undergoes hydrolysis to form a complex mixture of partially sulfomethylated derivatives, as well as colistin. Resistance to colistin began to appear as of 2015.

Carbapenems are a class of very effective antibiotic agents most commonly used for treatment of severe bacterial infections. This class of antibiotics is usually reserved for known or suspected multidrug-resistant (MDR) bacterial infections. Similar to penicillins and cephalosporins, carbapenems are members of the beta-lactam antibiotics drug class, which kill bacteria by binding to penicillin-binding proteins, thus inhibiting bacterial cell wall synthesis. However, these agents individually exhibit a broader spectrum of activity compared to most cephalosporins and penicillins. Furthermore, carbapenems are typically unaffected by emerging antibiotic resistance, even to other beta-lactams.

Acinetobacter baumannii is a typically short, almost round, rod-shaped (coccobacillus) Gram-negative bacterium. It is named after the bacteriologist Paul Baumann. It can be an opportunistic pathogen in humans, affecting people with compromised immune systems, and is becoming increasingly important as a hospital-derived (nosocomial) infection. While other species of the genus Acinetobacter are often found in soil samples, it is almost exclusively isolated from hospital environments. Although occasionally it has been found in environmental soil and water samples, its natural habitat is still not known.
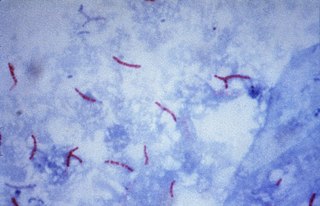
Multidrug-resistant tuberculosis (MDR-TB) is a form of tuberculosis (TB) infection caused by bacteria that are resistant to treatment with at least two of the most powerful first-line anti-TB medications (drugs): isoniazid and rifampin. Some forms of TB are also resistant to second-line medications, and are called extensively drug-resistant TB (XDR-TB).
Plasmid-mediated resistance is the transfer of antibiotic resistance genes which are carried on plasmids. Plasmids possess mechanisms that ensure their independent replication as well as those that regulate their replication number and guarantee stable inheritance during cell division. By the conjugation process, they can stimulate lateral transfer between bacteria from various genera and kingdoms. Numerous plasmids contain addiction-inducing systems that are typically based on toxin-antitoxin factors and capable of killing daughter cells that don't inherit the plasmid during cell division. Plasmids often carry multiple antibiotic resistance genes, contributing to the spread of multidrug-resistance (MDR). Antibiotic resistance mediated by MDR plasmids severely limits the treatment options for the infections caused by Gram-negative bacteria, especially family Enterobacteriaceae. The global spread of MDR plasmids has been enhanced by selective pressure from antimicrobial medications used in medical facilities and when raising animals for food.
Multidrug resistant Gram-negative bacteria are a type of Gram-negative bacteria with resistance to multiple antibiotics. They can cause bacteria infections that pose a serious and rapidly emerging threat for hospitalized patients and especially patients in intensive care units. Infections caused by MDR strains are correlated with increased morbidity, mortality, and prolonged hospitalization. Thus, not only do these bacteria pose a threat to global public health, but also create a significant burden to healthcare systems.
Carbapenem-resistant Enterobacteriaceae (CRE) or carbapenemase-producing Enterobacteriaceae (CPE) are Gram-negative bacteria that are resistant to the carbapenem class of antibiotics, considered the drugs of last resort for such infections. They are resistant because they produce an enzyme called a carbapenemase that disables the drug molecule. The resistance can vary from moderate to severe. Enterobacteriaceae are common commensals and infectious agents. Experts fear CRE as the new "superbug". The bacteria can kill up to half of patients who get bloodstream infections. Tom Frieden, former head of the Centers for Disease Control and Prevention has referred to CRE as "nightmare bacteria". Examples of enzymes found in certain types of CRE are KPC and NDM. KPC and NDM are enzymes that break down carbapenems and make them ineffective. Both of these enzymes, as well as the enzyme VIM have also been reported in Pseudomonas.
ESKAPE is an acronym comprising the scientific names of six highly virulent and antibiotic resistant bacterial pathogens including: Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp. The acronym is sometimes extended to ESKAPEE to include Escherichia coli. This group of Gram-positive and Gram-negative bacteria can evade or 'escape' commonly used antibiotics due to their increasing multi-drug resistance (MDR). As a result, throughout the world, they are the major cause of life-threatening nosocomial or hospital-acquired infections in immunocompromised and critically ill patients who are most at risk. P. aeruginosa and S. aureus are some of the most ubiquitous pathogens in biofilms found in healthcare. P. aeruginosa is a Gram-negative, rod-shaped bacterium, commonly found in the gut flora, soil, and water that can be spread directly or indirectly to patients in healthcare settings. The pathogen can also be spread in other locations through contamination, including surfaces, equipment, and hands. The opportunistic pathogen can cause hospitalized patients to have infections in the lungs, blood, urinary tract, and in other body regions after surgery. S. aureus is a Gram-positive, cocci-shaped bacterium, residing in the environment and on the skin and nose of many healthy individuals. The bacterium can cause skin and bone infections, pneumonia, and other types of potentially serious infections if it enters the body. S. aureus has also gained resistance to many antibiotic treatments, making healing difficult. Because of natural and unnatural selective pressures and factors, antibiotic resistance in bacteria usually emerges through genetic mutation or acquires antibiotic-resistant genes (ARGs) through horizontal gene transfer - a genetic exchange process by which antibiotic resistance can spread.
Cefiderocol, sold under the brand name Fetroja among others, is an antibiotic used to treat complicated urinary tract infections when no other options are available. It is indicated for the treatment of multi-drug-resistant Gram-negative bacteria including Pseudomonas aeruginosa. It is given by injection into a vein.
The Center for Innovative Phage Applications and Therapeutics (IPATH) is the first phage therapy center in North America, founded in the UC San Diego School of Medicine in June 2018, with seed funding from UC San Diego Chancellor Pradeep Khosla. The center was founded by Steffanie A. Strathdee and Robert "Chip" Schooley, both professors at UC San Diego School of Medicine. The center currently treats patients with life-threatening multi-drug resistant infections with phage therapy, on a case-by-case basis, through the Food and Drug Administration's (FDA's) compassionate use program. IPATH aims to initiate phase I/II phage therapy clinical trials, focusing on patients with cystic fibrosis and infections related to implantable hardware, such as pacemakers and prosthetic joints. The first planned clinical trial is set to look at otherwise healthy cystic fibrosis patients that are shedding Pseudomonas aeruginosa.

Corynebacterium striatum is a bacterium that is a member of the Corynebacterium genus. It is classified as non-diphtheritic. The bacterium is a gram-positive prokaryote that assumes a 'club-like' morphology, more formally known as a corynebacteria structure. It is non-lipophilic and undergoes aerobic respiration and is also a facultative anaerobe it is catalase negative and oxidase positive glucose and sucrose fermenter.

Robert "Chip" T. Schooley is an American infectious disease physician, who is the Vice Chair of Academic Affairs, Senior Director of International Initiatives, and Co-Director at the Center for Innovative Phage Applications and Therapeutics (IPATH), at the University of California San Diego School of Medicine. He is an expert in HIV and hepatitis C (HCV) infection and treatment, and in 2016, was the first physician to treat a patient in the United States with intravenous bacteriophage therapy for a systemic bacterial infection.

Multidrug-resistant bacteria are bacteria that are resistant to three or more classes of antimicrobial drugs. MDR bacteria have seen an increase in prevalence in recent years and pose serious risks to public health. MDR bacteria can be broken into 3 main categories: Gram-positive, Gram-negative, and other (acid-stain). These bacteria employ various adaptations to avoid or mitigate the damage done by antimicrobials. With increased access to modern medicine there has been a sharp increase in the amount of antibiotics consumed. Given the abundant use of antibiotics there has been a considerable increase in the evolution of antimicrobial resistance factors, now outpacing the development of new antibiotics.
References
- 1 2 3 4 A.-P. Magiorakos, A. Srinivasan, R. B. Carey, Y. Carmeli, M. E. Falagas, C. G. Giske, S. Harbarth, J. F. Hinndler et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria.... Clinical Microbiology and Infection, Vol 8, Iss. 3 first published 27 July 2011 [via Wiley Online Library]. Retrieved 16 August 2014.
- ↑ Drug+Resistance,+Multiple at the U.S. National Library of Medicine Medical Subject Headings (MeSH)
- ↑ Gall, Elizabeth; Long, Anna; Hall, Kendall K. (2020). "Infections Due to Other Multidrug-Resistant Organisms". Making Healthcare Safer III: A Critical Analysis of Existing and Emerging Patient Safety Practices. Rockville (MD): Agency for Healthcare Research and Quality (US). PMID 32255576.
- ↑ Boucher, HW, Talbot GH, Bradley JS, Edwards JE, Gilvert D, Rice LB, Schedul M., Spellberg B., Bartlett J. (1 January 2009). "Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America". Clinical Infectious Diseases. 48 (1): 1–12. doi: 10.1086/595011 . PMID 19035777.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ↑ Bennett PM (March 2008). "Plasmid encoded antibiotic resistance: acquisition and transfer of antibiotic resistance genes in bacteria". Br. J. Pharmacol. 153 (Suppl 1): S347–57. doi:10.1038/sj.bjp.0707607. PMC 2268074 . PMID 18193080.
- ↑ Reygaert, Wanda C. (2018). "An overview of the antimicrobial resistance mechanisms of bacteria". AIMS Microbiology. 4 (3): 482–501. doi:10.3934/microbiol.2018.3.482. ISSN 2471-1888. PMC 6604941 . PMID 31294229.
- ↑ Peterson, Elizabeth; Kaur, Parjit (2018). "Antibiotic Resistance Mechanisms in Bacteria: Relationships Between Resistance Determinants of Antibiotic Producers, Environmental Bacteria, and Clinical Pathogens". Frontiers in Microbiology. 9. doi: 10.3389/fmicb.2018.02928 . ISSN 1664-302X.
- ↑ Periasamy, Hariharan; Joshi, Prashant; Palwe, Snehal; Shrivastava, Rahul; Bhagwat, Sachin; Patel, Mahesh (10 February 2020). "High prevalence of Escherichia coli clinical isolates in India harbouring four amino acid inserts in PBP3 adversely impacting activity of aztreonam/avibactam". Journal of Antimicrobial Chemotherapy. 75 (6): 1650–1651. doi:10.1093/jac/dkaa021. ISSN 0305-7453. PMID 32040179.
- ↑ Li XZ, Nikaido H (August 2009). "Efflux-mediated drug resistance in bacteria: an update". Drugs. 69 (12): 1555–623. doi:10.2165/11317030-000000000-00000. PMC 2847397 . PMID 19678712.
- ↑ Stix G (April 2006). "An antibiotic resistance fighter". Sci. Am. 294 (4): 80–3. Bibcode:2006SciAm.294d..80S. doi:10.1038/scientificamerican0406-80. PMID 16596883.
- ↑ Hussain, T. Pakistan at the verge of potential epidemics by multi-drug resistant pathogenic bacteria (2015). Adv. Life Sci. 2(2). pp: 46-47
- ↑ Tao, Shuan; Chen, Huimin; Li, Na; Wang, Tong; Liang, Wei (2022). "The Spread of Antibiotic Resistance Genes In Vivo Model". Canadian Journal of Infectious Diseases and Medical Microbiology. 2022: e3348695. doi: 10.1155/2022/3348695 . ISSN 1712-9532. PMC 9314185 . PMID 35898691.
- ↑ Oechslin, Frank (30 June 2018). "Resistance Development to Bacteriophages Occurring during Bacteriophage Therapy". Viruses. 10 (7): 351. doi: 10.3390/v10070351 . PMC 6070868 . PMID 29966329.
- ↑ Howden BP, Slavin MA, Schwarer AP, Mijch AM (February 2003). "Successful control of disseminated Scedosporium prolificans infection with a combination of voriconazole and terbinafine". Eur. J. Clin. Microbiol. Infect. Dis. 22 (2): 111–3. doi:10.1007/s10096-002-0877-z. PMID 12627286. S2CID 29095136.
- ↑ Levin, Myron J.; Bacon, Teresa H.; Leary, Jeffry J. (2004). "Resistance of Herpes Simplex Virus Infections to Nucleoside Analogues in HIV‐Infected Patients". Clinical Infectious Diseases. 39 (s5): S248–S257. doi:10.1086/422364. ISSN 1058-4838. PMID 15494896.
- ↑ Dondorp, A., Nosten, F., Yi, P., Das, D., Phyo, A., & Tarning, J. et al. (2009). Artemisinin Resistance in Plasmodium falciparum Malaria. New England Journal Of Medicine, 361, 455-467.
- ↑ Doliwa C, Escotte-Binet S, Aubert D, Velard F, Schmid A, Geers R, Villena I. Induction of sulfadiazine resistance in vitro in Toxoplasma gondii.Exp Parasitol. 2013 Feb;133(2):131-6.
- ↑ Laurenson YC, Bishop SC, Forbes AB, Kyriazakis I.Modelling the short- and long-term impacts of drenching frequency and targeted selective treatment on the performance of grazing lambs and the emergence of antihelmintic resistance.Parasitology. 2013 Feb 1:1-12.
- ↑ Levy, Sharon (2014). "Reduced Antibiotic Use in Livestock: How Denmark Tackled Resistance". Environmental Health Perspectives. 122 (6): A160-5. doi:10.1289/ehp.122-A160. ISSN 0091-6765. PMC 4050507 . PMID 24892505.
- ↑ Schooley, Robert T.; Biswas, Biswajit; Gill, Jason J.; Hernandez-Morales, Adriana; Lancaster, Jacob; Lessor, Lauren; Barr, Jeremy J.; Reed, Sharon L.; Rohwer, Forest; Benler, Sean; Segall, Anca M.; Taplitz, Randy; Smith, Davey M.; Kerr, Kim; Kumaraswamy, Monika; Nizet, Victor; Lin, Leo; McCauley, Melanie D.; Strathdee, Steffanie A.; Benson, Constance A.; Pope, Robert K.; Leroux, Brian M.; Picel, Andrew C.; Mateczun, Alfred J.; Cilwa, Katherine E.; Regeimbal, James M.; Estrella, Luis A.; Wolfe, David M.; Henry, Matthew S.; Quinones, Javier; Salka, Scott; Bishop-Lilly, Kimberly A.; Young, Ry; Hamilton, Theron (14 August 2017). "Development and Use of Personalized Bacteriophage-Based Therapeutic Cocktails To Treat a Patient with a Disseminated Resistant Acinetobacter baumannii Infection". Antimicrobial Agents and Chemotherapy. American Society for Microbiology. 61 (10): e00954-17. doi:10.1128/aac.00954-17. ISSN 0066-4804. PMC 5610518 . PMID 28807909.