Related Research Articles

Blood pressure (BP) is the pressure of circulating blood against the walls of blood vessels. Most of this pressure results from the heart pumping blood through the circulatory system. When used without qualification, the term "blood pressure" refers to the pressure in a brachial artery, where it is most commonly measured. Blood pressure is usually expressed in terms of the systolic pressure over diastolic pressure in the cardiac cycle. It is measured in millimeters of mercury (mmHg) above the surrounding atmospheric pressure, or in kilopascals (kPa). The difference between the systolic and diastolic pressures is known as pulse pressure, while the average pressure during a cardiac cycle is known as mean arterial pressure.
Orthostatic hypotension, also known as postural hypotension, is a medical condition wherein a person's blood pressure drops when standing up or sitting down. Primary orthostatic hypotension is also often referred to as neurogenic orthostatic hypotension. The drop in blood pressure may be sudden, within 3 minutes or gradual. It is defined as a fall in systolic blood pressure of at least 20 mmHg or diastolic blood pressure of at least 10 mmHg after 3 minutes of standing. It occurs predominantly by delayed constriction of the lower body blood vessels, which is normally required to maintain adequate blood pressure when changing the position to standing. As a result, blood pools in the blood vessels of the legs for a longer period, and less is returned to the heart, thereby leading to a reduced cardiac output and inadequate blood flow to the brain.

Dysautonomia, autonomic failure, or autonomic dysfunction is a condition in which the autonomic nervous system (ANS) does not work properly. This may affect the functioning of the heart, bladder, intestines, sweat glands, pupils, and blood vessels. Dysautonomia has many causes, not all of which may be classified as neuropathic. A number of conditions can feature dysautonomia, such as Parkinson's disease, multiple system atrophy, dementia with Lewy bodies, Ehlers–Danlos syndromes, autoimmune autonomic ganglionopathy and autonomic neuropathy, HIV/AIDS, mitochondrial cytopathy, pure autonomic failure, autism, and postural orthostatic tachycardia syndrome.
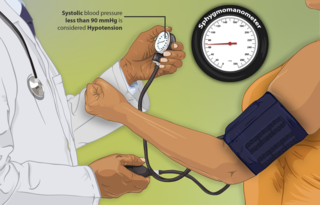
Hypotension is low blood pressure. Blood pressure is the force of blood pushing against the walls of the arteries as the heart pumps out blood. Blood pressure is indicated by two numbers, the systolic blood pressure and the diastolic blood pressure, which are the maximum and minimum blood pressures, respectively. A systolic blood pressure of less than 90 millimeters of mercury (mmHg) or diastolic of less than 60 mmHg is generally considered to be hypotension. Different numbers apply to children. However, in practice, blood pressure is considered too low only if noticeable symptoms are present.

Reflex syncope is a brief loss of consciousness due to a neurologically induced drop in blood pressure and/or a decrease in heart rate. Before an affected person passes out, there may be sweating, a decreased ability to see, or ringing in the ears. Occasionally, the person may twitch while unconscious. Complications of reflex syncope include injury due to a fall.

Hypovolemic shock is a form of shock caused by severe hypovolemia. It could be the result of severe dehydration through a variety of mechanisms or blood loss. Hypovolemic shock is a medical emergency; if left untreated, the insufficient blood flow can cause damage to organs, leading to multiple organ failure.
Orthostatic intolerance (OI) is the development of symptoms when standing upright that are relieved when reclining. There are many types of orthostatic intolerance. OI can be a subcategory of dysautonomia, a disorder of the autonomic nervous system occurring when an individual stands up. Some animal species with orthostatic hypotension have evolved to cope with orthostatic disturbances.

Postural orthostatic tachycardia syndrome (POTS) is a condition characterized by an abnormally large increase in heart rate upon sitting up or standing. POTS is a disorder of the autonomic nervous system that can lead the individual to experience a variety of symptoms. Symptoms may include lightheadedness, brain fog, blurred vision, weakness, fatigue, headaches, heart palpitations, exercise intolerance, nausea, diminished concentration, tremulousness (shaking), syncope (fainting), coldness or pain in the extremities, chest pain and shortness of breath. Other conditions associated with POTS include migraine headaches, Ehlers–Danlos syndrome, asthma, autoimmune disease,vasovagal syncope and mast cell activation syndrome. POTS symptoms may be treated with lifestyle changes such as increasing fluid and salt intake, wearing compression stockings, gentler and slow postural changes, avoiding prolonged bedrest, medication and physical therapy.

Neurogenic shock is a distributive type of shock resulting in hypotension, often with bradycardia, caused by disruption of autonomic nervous system pathways. It can occur after damage to the central nervous system, such as spinal cord injury and traumatic brain injury. Low blood pressure occurs due to decreased systemic vascular resistance resulting from loss of sympathetic tone, which in turn causes blood pooling within the extremities rather than being available to circulate throughout the body. The slowed heart rate results from a vagal response unopposed by a sympathetic nervous system (SNS) response. Such cardiovascular instability is exacerbated by hypoxia, or treatment with endotracheal or endobronchial suction used to prevent pulmonary aspiration.
Beck's triad is a collection of three medical signs associated with acute cardiac tamponade, a medical emergency when excessive fluid accumulates in the pericardial sac around the heart and impairs its ability to pump blood. The signs are low arterial blood pressure, distended neck veins, and distant, muffled heart sounds.

A tilt table test (TTT), occasionally called upright tilt testing (UTT), is a medical procedure often used to diagnose dysautonomia or syncope. Patients with symptoms of dizziness or lightheadedness, with or without a loss of consciousness (fainting), suspected to be associated with a drop in blood pressure or positional tachycardia are good candidates for this test.

A hypertensive emergency is very high blood pressure with potentially life-threatening symptoms and signs of acute damage to one or more organ systems. It is different from a hypertensive urgency by this additional evidence for impending irreversible hypertension-mediated organ damage (HMOD). Blood pressure is often above 200/120 mmHg, however there are no universally accepted cutoff values.

Droxidopa is a synthetic amino acid precursor which acts as a prodrug to the neurotransmitter norepinephrine (noradrenaline). Unlike norepinephrine, droxidopa is capable of crossing the protective blood–brain barrier (BBB).
The Bezold–Jarisch reflex involves a variety of cardiovascular and neurological processes which cause hypopnea, hypotension and bradycardia in response to noxious stimuli detected in the cardiac ventricles. The reflex is named after Albert von Bezold and Adolf Jarisch Junior. The significance of the discovery is that it was the first recognition of a chemical (non-mechanical) reflex.

Syncope, commonly known as fainting, or passing out, is a loss of consciousness and muscle strength characterized by a fast onset, short duration, and spontaneous recovery. It is caused by a decrease in blood flow to the brain, typically from low blood pressure. There are sometimes symptoms before the loss of consciousness such as lightheadedness, sweating, pale skin, blurred vision, nausea, vomiting, or feeling warm. Syncope may also be associated with a short episode of muscle twitching. Psychiatric causes can also be determined when a patient experiences fear, anxiety, or panic; particularly before a stressful event, usually medical in nature. When consciousness and muscle strength are not completely lost, it is called presyncope. It is recommended that presyncope be treated the same as syncope.

Orthostatic headache is a medical condition in which a person develops a headache while vertical and the headache is relieved when horizontal. Previously it was often misdiagnosed as different primary headache disorders such as migraine or tension headaches. Increasing awareness of the symptom and its causes has prevented delayed or missed diagnosis.

Dopamine beta (β)-hydroxylase deficiency is a condition involving inadequate dopamine beta-hydroxylase. It is characterized by increased amounts of serum dopamine and the absence of norepinephrine (NE) and epinephrine. Dopamine is released, as a false neurotransmitter, in place of norepinephrine. Other names for norepinephrine include noradrenaline (NA) and noradrenalin. This condition is also sometimes referred to as "norepinephrine deficiency". Researchers of disorders such as schizophrenia are interested in studying this disorder, as patients with these specific diseases can have an increase in the amount of dopamine in their system and yet do not show other symptoms of DβH deficiency.
Orthostatic hypertension is a medical condition consisting of a sudden and abrupt increase in blood pressure (BP) when a person stands up. Orthostatic hypertension is diagnosed by a rise in systolic BP of 20 mmHg or more when standing. Orthostatic diastolic hypertension is a condition in which the diastolic BP raises to 98 mmHg or over in response to standing, but this definition currently lacks clear medical consensus, so is subject to change. Orthostatic hypertension involving the systolic BP is known as systolic orthostatic hypertension.
Supine hypertension is a paradoxical elevation in blood pressure upon assuming a supine position from a standing or sitting position. It is assumed to be a manifestation of disorders of the autonomic nervous system or due to side effects of medications such as midodrine and droxidopa.
Adrenergic neurone blockers, commonly known as adrenergic antagonists, are a group of drugs that inhibit the sympathetic nervous system by blocking the activity of adrenergic neurones. They prevent the action or release of catecholamines such as norepinephrine and epinephrine. They are located throughout the body, causing various physiological reactions including bronchodilation, accelerated heartbeat, and vasoconstriction. They work by inhibiting the synthesis, release, or reuptake of the neurotransmitters or by antagonising the receptors on postsynaptic neurones. Their medical uses, mechanisms of action, adverse effects, and contraindications depend on the specific types of adrenergic blockers used, including alpha 1, alpha 2, beta 1, and beta 2.
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Momodu, Ifeanyi I.; Okafor, Chika N. (2019-01-01). "Orthostatic Syncope". NCBI Bookshelf. PMID 30725970 . Retrieved 2019-02-23.
- 1 2 3 Freeman, Roy; Wieling, Wouter; Axelrod, Felicia B.; Benditt, David G.; Benarroch, Eduardo; Biaggioni, Italo; Cheshire, William P.; Chelimsky, Thomas; Cortelli, Pietro; Gibbons, Christopher H.; Goldstein, David S.; Hainsworth, Roger; Hilz, Max J.; Jacob, Giris; Kaufmann, Horacio; Jordan, Jens; Lipsitz, Lewis A.; Levine, Benjamin D.; Low, Phillip A.; Mathias, Christopher; Raj, Satish R.; Robertson, David; Sandroni, Paola; Schatz, Irwin; Schondorff, Ron; Stewart, Julian M.; van Dijk, J. Gert (2011-03-24). "Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome". Clinical Autonomic Research. Springer Nature. 21 (2): 69–72. doi:10.1007/s10286-011-0119-5. ISSN 0959-9851. PMID 21431947. S2CID 11628648.
- 1 2 3 4 5 6 7 8 9 10 11 Nwazue, Victor C.; Raj, Satish R. (2013). "Confounders of Vasovagal Syncope". Cardiology Clinics. Elsevier BV. 31 (1): 89–100. doi:10.1016/j.ccl.2012.09.003. ISSN 0733-8651. PMC 3589989 . PMID 23217690.
- 1 2 3 4 5 6 Ali, Asad; Ali, Nouman Safdar; Waqas, Neha; Bhan, Chandur; Iftikhar, Waleed; Sapna, FNU; Jitidhar, FNU; Cheema, Abbas M; Ahmad, Malik Qistas; Nasir, Usama; Sami, Shahzad Ahmed; Zulfiqar, Annum; Ahmed, Asma (2018-08-20). "Management of Orthostatic Hypotension: A Literature Review". Cureus. Cureus, Inc. 10 (8): e3166. doi: 10.7759/cureus.3166 . ISSN 2168-8184. PMC 6197501 . PMID 30357001.
- ↑ Shen, Win-Kuang; Sheldon, Robert S.; Benditt, David G.; Cohen, Mitchell I.; Forman, Daniel E.; Goldberger, Zachary D.; Grubb, Blair P.; Hamdan, Mohamed H.; Krahn, Andrew D.; Link, Mark S.; Olshansky, Brian; Raj, Satish R.; Sandhu, Roopinder Kaur; Sorajja, Dan; Sun, Benjamin C.; Yancy, Clyde W. (2017-08-01). "2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society". Circulation. Ovid Technologies (Wolters Kluwer Health). 136 (5): e60–e122. doi: 10.1161/cir.0000000000000499 . ISSN 0009-7322. PMID 28280231.
- 1 2 Soteriades, Elpidoforos S.; Evans, Jane C.; Larson, Martin G.; Chen, Ming Hui; Chen, Leway; Benjamin, Emelia J.; Levy, Daniel (2002-09-19). "Incidence and Prognosis of Syncope". The New England Journal of Medicine. New England Journal of Medicine (NEJM/MMS). 347 (12): 878–885. doi: 10.1056/nejmoa012407 . ISSN 0028-4793. PMID 12239256.