The signs and symptoms of Graves' disease generally result from the direct and indirect effects of hyperthyroidism, although they can also be caused by other thyroidal conditions, such as Graves' ophthalmopathy, goitre and pretibial myxedema. These clinical manifestations can involve virtually every system in the body.
The mechanisms that mediate these effects are not well understood. The severity of the signs and symptoms of hyperthyroidism is related to the duration of the disease, the magnitude of the thyroid hormone excess, and the patient's age.
Although the majority of patients experience significant improvement and remission after proper medical care, health care providers should be aware of variability in individual response to hyperthyroidism and individual sensitivity to thyroid hormone fluctuations.[1] Patients with Graves' disease can also undergo periods of hypothyroidism (inadequate production of thyroid hormone; see symptoms of hypothyroidism), due to the challenges of finding the right dosage of thyroid hormone suppression and/or supplementation. The body's need for thyroid hormone can also change over time, such as in the first months after radioactive iodine treatment (RAI). Thyroid autoimmune diseases can also be volatile[citation needed], as hyperthyroidism can interchange with hypothyroidism and euthyroidism.[2]
Redness of the elbows is frequently present. It is probably the result of the combination of increased activity, an exposed part, and a hyperirritable vasomotor system.[4]
Tremor (usually fine shaking; tremor of the outstretched fingers). In a small study of newly diagnosed hyperthyroid patients, tremor was observed in 76% of them.[7] Some studies lay the cause for hyperthyroid tremor with a heightened beta-adrenergic state, others suggest an increased metabolism of dopamine.[8][9]
Weakness or muscle weakness (especially in the large muscles of the arms and legs). This latter occurs in 60 to 80 percent of patients with untreated hyperthyroidism.[10] Muscle weakness is rarely the chief complaint. The likelihood and degree of muscle weakness is correlated with the duration and severity of the hyperthyroid state, and becomes more likely after the age of 40. Muscle strength returns gradually over several months after the hyperthyroidism has been treated.
Muscle degeneration
Neurologic
A distinctly excessive reaction to all sorts of stimuli.[4]
A marked increase in fatigue, or asthenia, is often prominent. This increased weariness may be combined with hyperactivity; patients remark that they are impelled to incessant activity, which, however, causes great fatigue.[4]
Weight loss despite normal or increased appetite. Some patients (especially younger ones) gain weight due to excessive appetite stimulation that exceeds the weight loss effect.[11]
Augmented calcium levels in the blood (by as much as 25% – known as hypercalcaemia). This can cause stomach upset, excessive urination, and impaired kidney function.[13]
Diabetes may be activated or intensified, and its control worsened. The diabetes is ameliorated or may disappear when the thyrotoxicosis is treated.[4]
Reproductive symptoms in men may include reduced free testosterone (due to the elevation of testosterone-estrogen binding globulin level),[4] diminished libido, erectile dysfunction and (reversible) impaired sperm production with lower mean sperm density, a high incidence of sperm abnormalities, and reduced mobility of the sperm cells.[4]
Evidence of mild or severe liver disease may be found.[4]
Effects on the skeleton
Overt hyperthyroidism caused by Grave's Disease is associated with accelerated bone remodeling (resulting in increased porosity of cortical bone and reduced volume of trabecular bone). This can lead to reduced bone density and eventually osteoporosis as well as increased fracture rates. The increased hip fracture rates later in life in turn cause excess late mortality.[citation needed] The changes in bone metabolism are connected with negative calcium balance, an increased excretion of calcium and phosphorus in the urine (hypercalciuria) and stool, and, rarely, hypercalcemia.[13] In hyperthyroidism, the normal cycle duration of bone resorption of approximately 200 days is halved, and each cycle is associated with a 9.6 percent loss of mineralized bone. In hypothyroidism, cycle length approximates 700 days and is associated with a 17 percent increase in mineralized bone.[17]
The extent of the reduction in bone density in most studies is 10–20%. The clinical manifestations on bone differ depending on the age of the patient. Postmenopausal woman are most sensitive to accelerated bone loss from thyrotoxicosis. Accelerated bone growth in growing children can increase ossification in the short term, but generally results in short-stature adults compared with the predicted heights.[citation needed]
If thyrotoxicosis is treated early, bone loss can be minimized.[13] The level of calcium in the blood can be determined by a simple blood test, and a Dual Energy X-Ray Absorptiometry scan can help determine patient bone density relative to the rest of the population. There are many medications that can help to rebuild bone mass and to prevent further bone loss, such as Bisphosphonates.[13]Risedronate treatment has been demonstrated to help restore bone mass in osteopenia/osteoporosis associated with Graves' disease.[18] Nevertheless, weight-bearing exercises, a balanced diet, calcium intake of about 1500mg a day and enough vitamin D, are of course elementary foundations.[13]
Eye symptoms
Hyperthyroidism almost always causes general eye symptoms like dryness and irritation, regardless of what the cause of the hyperthyroid state is. However, these need to be distinguished from Graves' ophthalmopathy, which can only occur in patients who have Graves' disease. (It may also, rarely, be seen in Hashimoto's thyroiditis, primary hypothyroidism, and thyroid cancer).[19]
About 20–25% of patients with Graves' disease will suffer from clinically obvious Graves' ophthalmopathy, and not just from the eye signs of hyperthyroidism. Only 3 to 5% will develop severe ophthalmopathy.[20] However, when subjected to closer inspection (e.g. by magnetic resonance imaging of the orbits) many more patients have evidence of ophthalmopathy. It is estimated that for every 100,000 persons, 16 women and 3 men have Graves' ophthalmopathy every year.[21]
Although it is true that in most patients ophthalmopathy, goiter, and symptoms of thyrotoxicosis appear more or less coincidentally, it is also true that in certain cases eye signs may appear long before thyrotoxicosis is evident, or become worse when the thyrotoxicosis is subsiding or has been controlled by treatment.[4] In approximately 20% of ophthalmopathy patients, ophthalmopathy appears before the onset of hyperthyroidism, in about 40% concurrently, and in about 20% in the six months after diagnosis.[22] In the remainder, the eye disease first becomes apparent after treatment of the hyperthyroidism, more often in patients treated with radioiodine.[23]
It can sometimes be difficult to distinguish between eye symptoms due to hyperthyroidism and those due to Graves' antibodies, because the two often occur coincidentally. What can make things particularly difficult, is that many patients with hyperthyroidism have lid retraction, which leads to stare and lid lag (due to contraction of the levator palpebrae muscles of the eyelids). This stare may then give the appearance of protruding eyeballs (proptosis), when none in fact exists. This subsides when the hyperthyroidism is treated.[citation needed]
Photo showing the classic finding of proptosis and lid retraction in Graves' disease
Graves' ophthalmopathy is characterized by inflammation of the extraocular muscles, orbital fat and connective tissue. It results in the following signs, which can be extremely distressing to the patient:[4]
Most frequent are symptoms due to conjunctival or corneal irritation: burning, photophobia, tearing, pain, and a gritty or sandy sensation.[4]
Several studies have suggested a high prevalence of neuropsychiatric disorders and mental disorder symptoms in Graves' disease (and thyroid disease in general), which are similar to those in patients with organic brain disease.[25][26][27][28][29] These manifestations are diverse, affecting the central and peripheral nervous systems. The vast majority of patients with hyperthyroidism meet criteria for some psychiatric disorders,[25] and those with milder presentations are probably not entirely free of mental symptoms such as emotional lability, tension, depression and anxiety.[25] Anxiety syndromes related to hyperthyroidism are typically complicated by major depression and cognitive decline, such as in memory and attention.[30] Some studies contradict the psychological findings. For example, a large 2002 study found "no statistical association between thyroid dysfunction, and the presence of depression or anxiety disorder."[31] In one study on hospitalised elderly patients, over half had cognitive impairment with either dementia or confusion.[32] However, a controlled study on 31 Graves' disease patients found that while patients had subjective reports of cognitive deficits in the toxic phase of Graves' thyrotoxicosis, formal testing found no cognitive impairment and suggested the reported symptoms may reflect the affective and somatic manifestations of hyperthyroidism.[33] Notably, a literature review of 2006 notes methodology issues in the consistency of Graves' disease diagnostic criteria, which might explain the apparently contradicting findings. These researchers found many reports about residual complaints in patients who were euthyroid after treatment, with a high prevalence of anxiety disorders and bipolar disorder, as well as elevated scores on scales of anxiety, depression and psychological distress.[25] In a 1992 study, a significant proportion of the 137 questioned patients with Graves' disease reported – among other things – increased crying (55%), being easily startled (53%), being tired all the time (47%), a significant decrease in social activity (46%), feelings of being out of control (45%), feelings of hopelessness (43%), loss of sense of humor (41%), loss of interest in things they formerly enjoyed (39%), not being able to 'connect' with others (34%).[34]
Several studies point out that the severity of psychiatric symptoms could easily result in an inappropriate referral to a psychiatrist prior to the diagnosis of hyperthyroidism.[35][36] Consequently, undiagnosed hyperthyroidism sometimes results in inappropriate use of psychotropic medications; prompt recognition of hyperthyroidism (or hypothyroidism) through thyroid function screening is therefore recommended in the evaluation of patients with psychiatric symptoms.[36][37] Naturally, the management of patients would be improved by collaboration between an endocrinologist and a psychiatrist.[38]
Overall, reported symptoms vary from mild to severe aspects of anxiety or depression, and may include psychotic and behavioral disturbances:
The pathological well-being (euphoria) or hyperactivity may produce a state of exhaustion, and profound fatigue or asthenia chiefly characterizes the picture.[4]
Erratic behaviour may include intermittent rage disorder and mild attention deficit disorder.[43] Some patients become hyperirritable and combative, which can precipitate accidents or even assaultive behaviour.[4]
In more extreme cases features of psychosis,[44] with delusions of persecution or delusions of reference,[45] and pressure of speech may present themselves. Rarely, patients develop visual or auditory hallucinations or a frank psychosis,[4] and may appear schizophrenic, lose touch with reality and become delirious,[2][39] Such psychotic symptoms may not completely clear up after the hyperthyroidism has been treated.[4] Paranoia and paranoid-hallucinatory psychosis in hyperthyroidism usually have a manic disposition and it is therefore often not clear if the patient is experiencing a paranoid psychosis with depressive streaks, or a depression that has paranoid streaks.[2]
Treatment of hyperthyroidism typically leads to improvement in cognitive and behavioral impairments.[33] Agitation, inattention, and frontal lobe impairment may improve more rapidly than other cognitive functions. However, several studies confirm that a substantial proportion of patients with hyperthyroidism have psychiatric disorders or mental symptoms and decreased quality of life even after successful treatment of their hyperthyroidism.[27]
Effects on pre-existing psychiatric disorders
Patients with pre-existing psychiatric disorders, will experience a worsening of their usual symptoms, as observed by several studies. A study of 1999 found that Graves' disease exacerbated the symptoms of Tourette's disorder and attention-deficit hyperactivity disorder (ADHD), and points out that the lack of diagnosis of the Graves' disease compromised the efficacy of the treatment of these disorders.[46] Patients who are known to have a convulsive disorder may become more difficult to control with the usual medications, and seizures may appear in patients who have never previously manifested such symptoms.[4]
Sub-clinical hyperthyroidism
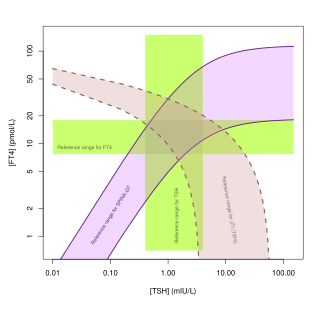
In sub-clinical hyperthyroidism, serum TSH is abnormally low, but T4- and T3-levels fall within laboratory reference ranges.[47] It primarily affects the skeleton and the cardiovascular system (abnormalities in other systems have also been reported), in a similar but less severe and less frequent way than overt hyperthyroidism does. It can alter cardiac function, with increased heart rate, increased left ventricular mass index, increased cardiac contractility, diastolic dysfunction, and induction of ectopic atrial beats. Long-term mild excess of thyroid hormone can thus cause impaired cardiac reserve and exercise capacity.[4] In a large population-based study of 2008, the odds of having poorer cognitive function were greater for sub-clinical hyperthyroidism than for stroke, diabetes mellitus, and Parkinson's disease.[48] Sub-clinical hyperthyroidism might modestly increase the risk of cognitive impairment and dementia.[49] Subclinical hyperthyroidism in pregnancy is associated with an increased risk of pre-eclampsia, low birth weight, miscarriage and preterm birth.[50]Propylthiouracil is the preferred treatment of hyperthyroidism (both overt and subclinical) in the first trimester of pregnancy as it is associated with less birth defects than methimazole.[50]
A possible explanation for the mental symptoms of sub-clinical thyroid disease, might be found in the fact that the brain has among the highest expression of THR's[clarification needed], and that neurons are often more sensitive than other tissues to thyroid abnormalities, including sub-clinical hyperthyroidism and thyrotoxicosis.[51][52][53] In a 1996 survey study respondents reported a significant decline in memory, attention, planning, and overall productivity from the period 2 years prior to Graves' symptoms onset to the period when hyperthyroid.[27] Also, hypersensitivity of the central nervous system to low-grade hyperthyroidism can result in an anxiety disorder before other Graves' disease symptoms emerge. E.g., panic disorder has been reported to precede Graves' hyperthyroidism by 4 to 5 years in some cases, although it is not known how frequently this occurs.[54]
However, while clinical hyperthyroidism is associated with frank neuropsychological and affective alterations, the occurrence of these alterations and their treatment in mild and sub-clinical hyperthyroidism remains a controversial issue. Regardless of the inconsistent findings, a 2007 study by Andersen et al. states that the distinction between sub-clinical and overt thyroid disease is in any case somewhat arbitrary.[55] Sub-clinical hyperthyroidism has been reported in 63% of euthyroid Graves' disease,[56] but only in 4% of cases where Graves' disease was in remission.[57]
Subclinical hyperthyroidism has an 8% risk of converting to overt hyperthyroidism at 1 year, and a 26% risk at 5 years.[50]
Children and adolescents
Hyperthyroidism has unique effects in children on growth and pubertal development, e.g. causing epiphyseal maturation. In growing children, accelerated bone growth from hyperthyroidism can increase osteogenesis in the short term, but generally results in short-stature adults compared with the predicted heights. Pubertal development tends to be delayed, or slowed. Girls who have undergone menarche may develop secondary amenorrhea. Hyperthyroidism is associated with high sex hormone-binding globulin (SHBG), which may result in high serum estradiol levels in girls and testosterone levels in boys. However, unbound or free levels of these hormones are decreased. Hyperthyroidism before the age of four may cause neurodevelopmental delay. A study by Segni et al. suggests that permanent brain damage can occur as a result of the illness.[4][58]
Ophthalmopatic findings are more common but less severe in children (severe infiltrative exophthalmos is virtually unknown before mid-adolescence), but besides that, many of the typical clinical features of hyperthyroidism in children and adolescents are similar to those in adults.[4] An important difference between children and adults with Graves' disease, is that children have not yet developed like adults have (psychological and physiological), and that they are a lot more dependent on their environment. The encephalopathy will have profound effects on children's developing personalities and developing relationship with their environment. Disturbments in bodily development further complicates matters. The consequences for the development and the somatic and psychological well-being of the child can be very radical and sometimes irreversible. The earlier a person is affected by thyroid disease, the more the development of personality is affected and the bigger the delay from their potential development level. The child gets behind in its cognitive, emotional and sexual growth, which, by itself, also influences its processing abilities of the endocrine disease.[2]
Children with hyperthyroidism tend to have greater mood swings and disturbances of behavior, as compared with adults. Their attention span decreases, they are usually hyperactive and distractible, they sleep poorly, and their school performance deteriorates. Because devastating personality and emotional changes often appear in the child or adolescent with Graves' disease, many hyperthyroid children are (similar to many adults) referred to a developmental specialist or child psychiatrist before the presence of hyperthyroidism is suspected.[4]
Older patients
In older patients, emotional instability may be less evident, or depression may occur, and the symptoms and signs are manifestly circulatory. In many, the thyroid is not readily palpable.[4] Symptoms such as rapid heart rate, shortness of breath on exertion, and edema may predominate. Older patients also tend to have more weight loss and less of an increase in appetite. Thus anorexia in this group is fairly frequent, as is constipation.[4] Elderly patients may have what is called "apathetic thyrotoxicosis", a state in which they have less and less severe symptoms, except for weakness, depression and lethargy (making it even more prone to escape diagnosis).[citation needed]
Graves' disease and work
Considering the many signs and symptoms, the generally delayed diagnosis, and the possibility of residual complaints after treatment, it is little wonder that a significant number of people with Graves' disease have difficulty keeping their job. One study found that of 303 patients successfully treated for hyperthyroidism (77% had Graves' disease) 53% dealt with lack of energy. About one-third were unable to resume their customary work, mainly due to persistent mental problems.[25][59] In their 1986 study of 26 patients (10 years after successful treatment of hyperthyroidism), Perrild et al. note that four patients had been granted disability pensions on the basis of intellectual dysfunction.[60] Between 2006 and 2008, Ponto et al. surveyed 250 Graves' disease patients. Of these, 36% were written off sick and 5% even had to take early retirement. In the same study, 34% of 400 questioned physicians reported treating patients with fully impaired earning capacity.[61]
Patients can and do recover with appropriate therapy while continuing to work, but more rapid and certain progress is made if a period away from the usual occupation can be provided.[18] Two important considerations are adequate rest and attention to nutrition.[18]
Related Research Articles
Hyperthyroidism is the condition that occurs due to excessive production of thyroid hormones by the thyroid gland. Thyrotoxicosis is the condition that occurs due to excessive thyroid hormone of any cause and therefore includes hyperthyroidism. Some, however, use the terms interchangeably. Signs and symptoms vary between people and may include irritability, muscle weakness, sleeping problems, a fast heartbeat, heat intolerance, diarrhea, enlargement of the thyroid, hand tremor, and weight loss. Symptoms are typically less severe in the elderly and during pregnancy. An uncommon but life-threatening complication is thyroid storm in which an event such as an infection results in worsening symptoms such as confusion and a high temperature; this often results in death. The opposite is hypothyroidism, when the thyroid gland does not make enough thyroid hormone.
Graves' disease, also known as toxic diffuse goiter, is an autoimmune disease that affects the thyroid. It frequently results in and is the most common cause of hyperthyroidism. It also often results in an enlarged thyroid. Signs and symptoms of hyperthyroidism may include irritability, muscle weakness, sleeping problems, a fast heartbeat, poor tolerance of heat, diarrhea and unintentional weight loss. Other symptoms may include thickening of the skin on the shins, known as pretibial myxedema, and eye bulging, a condition caused by Graves' ophthalmopathy. About 25 to 30% of people with the condition develop eye problems.
Premenstrual dysphoric disorder (PMDD) is a mood disorder characterized by emotional, cognitive, and physical symptoms. PMDD causes significant distress or impairment in menstruating people during the luteal phase of the menstrual cycle. The symptoms occur in the luteal phase, improve within a few days after the onset of menses, and are minimal or absent in the week after menses. PMDD has a profound impact on a person's quality of life and dramatically increases the risk of suicidal ideation and even suicide attempts. Many women of reproductive age experience discomfort or mild mood changes prior to menstruation. However, 5–8% experience severe premenstrual syndrome causing significant distress or functional impairment. Within this population of reproductive age, some will meet the criteria for PMDD.
Hashimoto's thyroiditis, also known as chronic lymphocytic thyroiditis and Hashimoto's disease, is an autoimmune disease in which the thyroid gland is gradually destroyed. A slightly broader term is autoimmune thyroiditis, identical other than that it is also used to describe a similar condition without a goiter.
Thyroid disease is a medical condition that affects the function of the thyroid gland. The thyroid gland is located at the front of the neck and produces thyroid hormones that travel through the blood to help regulate many other organs, meaning that it is an endocrine organ. These hormones normally act in the body to regulate energy use, infant development, and childhood development.
Thyroiditis is the inflammation of the thyroid gland. The thyroid gland is located on the front of the neck below the laryngeal prominence, and makes hormones that control metabolism.
Toxic multinodular goiter (TMNG), also known as multinodular toxic goiter (MNTG), is an active multinodular goiter associated with hyperthyroidism.
Thyroid storm is a rare but severe and life-threatening complication of hyperthyroidism. It occurs when an overactive thyroid leads to hypermetabolism, which can cause death from cardiac arrest or multiple organ failure.
Pretibial myxedema is an infiltrative dermopathy, resulting as a rare complication of Graves' disease, with an incidence rate of about 1–5%.
Liothyronine is a manufactured form of the thyroid hormone triiodothyronine (T3). It is most commonly used to treat hypothyroidism and myxedema coma. It can be taken by mouth or by injection into a vein.
De Quervain's thyroiditis, also known as subacute granulomatous thyroiditis or giant cell thyroiditis, is a member of the group of thyroiditis conditions known as resolving thyroiditis. People of all ages and genders may be affected.
Graves’ ophthalmopathy, also known as thyroid eye disease (TED), is an autoimmune inflammatory disorder of the orbit and periorbital tissues, characterized by upper eyelid retraction, lid lag, swelling, redness (erythema), conjunctivitis, and bulging eyes (exophthalmos). It occurs most commonly in individuals with Graves' disease, and less commonly in individuals with Hashimoto's thyroiditis, or in those who are euthyroid.
Euthyroid sick syndrome (ESS) is a state of adaptation or dysregulation of thyrotropic feedback control wherein the levels of T3 and/or T4 are abnormal, but the thyroid gland does not appear to be dysfunctional. This condition may result from allostatic responses of hypothalamus-pituitary-thyroid feedback control, dyshomeostatic disorders, drug interferences, and impaired assay characteristics in critical illness.
Thyrotoxicosis factitia is a condition of thyrotoxicosis caused by the ingestion of exogenous thyroid hormone. It can be the result of mistaken ingestion of excess drugs, such as levothyroxine and triiodothyronine, or as a symptom of Munchausen syndrome. It is an uncommon form of hyperthyroidism.
Thyroid hormones are any hormones produced and released by the thyroid gland, namely triiodothyronine (T3) and thyroxine (T4). They are tyrosine-based hormones that are primarily responsible for regulation of metabolism. T3 and T4 are partially composed of iodine, derived from food. A deficiency of iodine leads to decreased production of T3 and T4, enlarges the thyroid tissue and will cause the disease known as simple goitre.
Thyrotoxic periodic paralysis (TPP) is a rare condition featuring attacks of muscle weakness in the presence of hyperthyroidism. Hypokalemia is usually present during attacks. The condition may be life-threatening if weakness of the breathing muscles leads to respiratory failure, or if the low potassium levels lead to abnormal heart rhythms. If untreated, it is typically recurrent in nature.
Thyroid disease in pregnancy can affect the health of the mother as well as the child before and after delivery. Thyroid disorders are prevalent in women of child-bearing age and for this reason commonly present as a pre-existing disease in pregnancy, or after childbirth. Uncorrected thyroid dysfunction in pregnancy has adverse effects on fetal and maternal well-being. The deleterious effects of thyroid dysfunction can also extend beyond pregnancy and delivery to affect neurointellectual development in the early life of the child. Due to an increase in thyroxine binding globulin, an increase in placental type 3 deioidinase and the placental transfer of maternal thyroxine to the fetus, the demand for thyroid hormones is increased during pregnancy. The necessary increase in thyroid hormone production is facilitated by high human chorionic gonadotropin (hCG) concentrations, which bind the TSH receptor and stimulate the maternal thyroid to increase maternal thyroid hormone concentrations by roughly 50%. If the necessary increase in thyroid function cannot be met, this may cause a previously unnoticed (mild) thyroid disorder to worsen and become evident as gestational thyroid disease. Currently, there is not enough evidence to suggest that screening for thyroid dysfunction is beneficial, especially since treatment thyroid hormone supplementation may come with a risk of overtreatment. After women give birth, about 5% develop postpartum thyroiditis which can occur up to nine months afterwards. This is characterized by a short period of hyperthyroidism followed by a period of hypothyroidism; 20–40% remain permanently hypothyroid.
Thyroid's secretory capacity is the maximum stimulated amount of thyroxine that the thyroid can produce in a given time-unit.
The sum activity of peripheral deiodinases is the maximum amount of triiodothyronine produced per time-unit under conditions of substrate saturation. It is assumed to reflect the activity of deiodinases outside the central nervous system and other isolated compartments. GD is therefore expected to reflect predominantly the activity of type I deiodinase.
Amiodarone induced thyrotoxicosis (AIT) is a form of hyperthyroidism due to treatment with antiarrhythmic drug, amiodarone.
References
↑ Druckerhttp D (2005). "Hyperthyroidism". MyThyroid.com. Retrieved 2010-05-03.
1 2 3 4 Psychische stoornissen bij endocriene zieken, 1983, C. van der Meer en W. van Tilburg (red.)
↑ Cutaneous manifestations of thyroid disease. Heymann WR, J Am Acad Dermatol. 1992;26(6) 885.
↑ Surgical management of multinodular goiter with compression symptoms. Ríos A, Rodríguez JM, Canteras M, Galindo PJ, Tebar FJ, Parrilla P, Arch Surg. 2005;140(1) 49; Compression syndromes caused by substernal goitres. Anders HJ, Postgrad Med J. 1998;74(872) 327.
↑ Henderson JM, Portmann L, Van Melle G, Haller E, Ghika JA (1997). "Propranolol as an adjunct therapy for hyperthyroid tremor". European Neurology. 37 (3): 182–5. doi:10.1159/000117431. PMID9137929.
↑ Neuromuscular findings in thyroid dysfunction: a prospective clinical and electrodiagnostic study. Duyff RF, Van den Bosch J, Laman DM, van Loon BJ, Linssen WH, J Neurol Neurosurg Psychiatry. 2000;68(6) 750; Electromyographic and histological findings in the muscles of patients with thyrotoxicosis. HAVARD CW, CAMPBELL ED, ROSS HB, SPENCE AW, Q J Med. 1963;32:145; Electromyography in thyrotoxicosis. Ramsay ID, Q J Med. 1965;34(135) 255.
↑ Gleicher N, Weghofer A, Barad DH (Apr 2011). "Do chromosomally abnormal pregnancies really preclude autoimmune etiologies of spontaneous miscarriages?". Autoimmunity Reviews. 10 (6): 361–3. doi:10.1016/j.autrev.2010.12.004. PMID21195806.
↑ Gleicher N (December 2010). "Does the immune system induce labor? Lessons from preterm deliveries in women with autoimmune diseases". Clinical Reviews in Allergy & Immunology. 39 (3): 194–206. doi:10.1007/s12016-009-8180-8. PMID19844811. S2CID37559462.
↑ A survey study of neuropsychiatric complaints in patients with Graves' disease. Stern RA, Robinson B, Thorner AR, Arruda JE, Prohaska ML, Prange AJ Jr, J Neuropsychiatry Clin Neurosci. 1996;8(2) 181.
↑ Normal and pathological remodeling of human trabecular bone: three dimensional reconstruction of the remodeling sequence in normals and in metabolic bone disease. Eriksen EF, Endocr Rev. 1986;7(4) 379.
↑ Graves' ophthalmopathy: a preventable disease? Luigi Bartalena, Claudio Marcocci and Aldo Pinchera1 – European Journal of Endocrinology (2002) 146 457–461
↑ Bartley GB, Fatourechi V, Kadrmas EF, Jacobsen SJ, Ilstrup DM, Garrity JA, Gorman CA (1995). "The incidence of Graves' ophthalmopathy in Olmsted County, Minnesota". American Journal of Ophthalmology. 120 (4): 511–7. doi:10.1016/s0002-9394(14)72666-2. PMID7573310.
↑ Bartley GB, Fatourechi V, Kadrmas EF, Jacobsen SJ, Ilstrup DM, Garrity JA, Gorman CA (1996). "Chronology of Graves' ophthalmopathy in an incidence cohort". American Journal of Ophthalmology. 121 (4): 426–34. doi:10.1016/S0002-9394(14)70439-8. PMID8604736.
↑ Trzepacz PT, McCue M, Klein I, Levey GS, Greenhouse J (1988). "A psychiatric and neuropsychological study of patients with untreated Graves' disease". General Hospital Psychiatry. 10 (1): 49–55. doi:10.1016/0163-8343(88)90084-9. PMID3345907.
↑ Engum A, Bjøro T, Mykletun A, Dahl AA; Bjøro; Mykletun; Dahl (July 2002). "An association between depression, anxiety and thyroid function--a clinical fact or an artifact?". Acta Psychiatrica Scandinavica. 106 (1): 27–34. doi:10.1034/j.1600-0447.2002.01250.x. PMID12100345. S2CID46316229.{{cite journal}}: CS1 maint: multiple names: authors list (link)
1 2 Vogel A, Elberling TV, Hørding M, etal. (January 2007). "Affective symptoms and cognitive functions in the acute phase of Graves' thyrotoxicosis". Psychoneuroendocrinology. 32 (1): 36–43. doi:10.1016/j.psyneuen.2006.09.012. PMID17097812. S2CID54416080.
↑ Journal of Neuropsychiatry and clinical neurosciences, 1996, 8:181–185.
↑ Trzepacz PT, McCue M, Klein I, Levey GS, Greenhouse J; McCue; Klein; Levey; Greenhouse (January 1988). "A psychiatric and neuropsychological study of patients with untreated Graves' disease". General Hospital Psychiatry. 10 (1): 49–55. doi:10.1016/0163-8343(88)90084-9. PMID3345907.{{cite journal}}: CS1 maint: multiple names: authors list (link)
1 2 McGaffee J, Lippmann S, Barnes MA; Lippmann; Barnes (February 1983). "Psychiatric presentations of hyperthyroidism". American Family Physician. 27 (2): 257–60. PMID6687506.{{cite journal}}: CS1 maint: multiple names: authors list (link)
↑ Psychiatric Manifestations of Graves' Hyperthyroidism Pathophysiology and Treatment Options Robertas Bunevicius and Arthur J. Prange Jr – CNS Drugs. 2006;20(11) 897–909
↑ Psychische stoornissen bij endocriene zieken, 1983, C. van der Meer en W. van Tilburg (red.) suggests usually with an agitated streak, not a depression of the inhibited type
↑ Bunevicius R, Velickiene D, Prange AJ; Velickiene; Prange Jr (2005). "Mood and anxiety disorders in women with treated hyperthyroidism and ophthalmopathy caused by Graves' disease". General Hospital Psychiatry. 27 (2): 133–9. doi:10.1016/j.genhosppsych.2004.10.002. PMID15763125.{{cite journal}}: CS1 maint: multiple names: authors list (link)
↑ Narrow Individual Variations in Serum T4 and T3 in Normal Subjects: A Clue to the Understanding of Subclinical Thyroid Disease Stig Andersen, Klaus Michael Pedersen, Niels Henrik Bruun and Peter Laurberg – The Journal of Clinical Endocrinology & Metabolism, 2007, Vol. 87, No. 3 1068–1072
↑ Studies on thyrotrophin receptor antibodies in patients with euthyroid Graves' disease. Kasagi K, Hatabu H, Tokuda Y, Iida Y, Endo K, Konishi J, Clin Endocrinol. 1988;29(4) 357.
↑ Studies of thyroid function and immune parameters in patients with hyperthyroid Graves' disease in remission. Murakami M, Koizumi Y, Aizawa T, Yamada T, Takahashi Y, Watanabe T, Kamoi K, The Journal of Clinical Endocrinology and Metabolism 1988;66(1) 103.
↑ Segni M, Leonardi E, Mazzoncini B, Pucarelli I, Pasquino AM; Leonardi; Mazzoncini; Pucarelli; Pasquino (1999). "Special features of Graves' disease in early childhood". Thyroid. 9 (9): 871–7. doi:10.1089/thy.1999.9.871. PMID10524565.{{cite journal}}: CS1 maint: multiple names: authors list (link)
↑ Fahrenfort JJ, Wilterdink AM, van der Veen EA; Wilterdink; Van Der Veen (2000). "Long-term residual complaints and psychosocial sequelae after remission of hyperthyroidism". Psychoneuroendocrinology. 25 (2): 201–11. doi:10.1016/S0306-4530(99)00050-5. PMID10674283. S2CID25205989.{{cite journal}}: CS1 maint: multiple names: authors list (link)
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.