A Colles' fracture is a type of fracture of the distal forearm in which the broken end of the radius is bent backwards. Symptoms may include pain, swelling, deformity, and bruising. Complications may include damage to the median nerve.

A joint dislocation, also called luxation, occurs when there is an abnormal separation in the joint, where two or more bones meet. A partial dislocation is referred to as a subluxation. Dislocations are often caused by sudden trauma on the joint like an impact or fall. A joint dislocation can cause damage to the surrounding ligaments, tendons, muscles, and nerves. Dislocations can occur in any major joint or minor joint. The most common joint dislocation is a shoulder dislocation.
A distal radius fracture, also known as wrist fracture, is a break of the part of the radius bone which is close to the wrist. Symptoms include pain, bruising, and rapid-onset swelling. The ulna bone may also be broken.
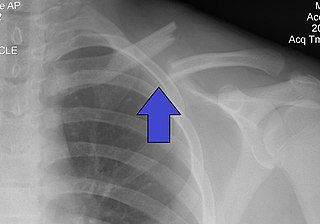
A clavicle fracture, also known as a broken collarbone, is a bone fracture of the clavicle. Symptoms typically include pain at the site of the break and a decreased ability to move the affected arm. Complications can include a collection of air in the pleural space surrounding the lung (pneumothorax), injury to the nerves or blood vessels in the area, and an unpleasant appearance.

A hip fracture is a break that occurs in the upper part of the femur, at the femoral neck or (rarely) the femoral head. Symptoms may include pain around the hip, particularly with movement, and shortening of the leg. Usually the person cannot walk.

An avulsion fracture is a bone fracture which occurs when a fragment of bone tears away from the main mass of bone as a result of physical trauma. This can occur at the ligament by the application of forces external to the body or at the tendon by a muscular contraction that is stronger than the forces holding the bone together. Generally muscular avulsion is prevented by the neurological limitations placed on muscle contractions. Highly trained athletes can overcome this neurological inhibition of strength and produce a much greater force output capable of breaking or avulsing a bone.

A hip dislocation is when the thighbone (femur) separates from the hip bone (pelvis). Specifically it is when the ball–shaped head of the femur separates from its cup–shaped socket in the hip bone, known as the acetabulum. The joint of the femur and pelvis is very stable, secured by both bony and soft-tissue constraints. With that, dislocation would require significant force which typically results from significant trauma such as from a motor vehicle collision or from a fall from elevation. Hip dislocations can also occur following a hip replacement or from a developmental abnormality known as hip dysplasia.
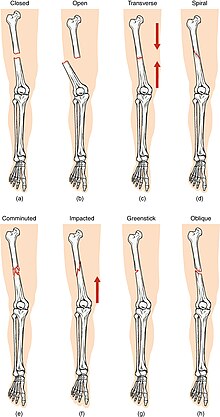
An open fracture, also called a compound fracture, is a type of bone fracture that has an open wound in the skin near the fractured bone. The skin wound is usually caused by the bone breaking through the surface of the skin. An open fracture can be life threatening or limb-threatening due to the risk of a deep infection and/or bleeding. Open fractures are often caused by high energy trauma such as road traffic accidents and are associated with a high degree of damage to the bone and nearby soft tissue. Other potential complications include nerve damage or impaired bone healing, including malunion or nonunion. The severity of open fractures can vary. For diagnosing and classifying open fractures, Gustilo-Anderson open fracture classification is the most commonly used method. This classification system can also be used to guide treatment, and to predict clinical outcomes. Advanced trauma life support is the first line of action in dealing with open fractures and to rule out other life-threatening condition in cases of trauma. The person is also administered antibiotics for at least 24 hours to reduce the risk of an infection.

A humerus fracture is a break of the humerus bone in the upper arm. Symptoms may include pain, swelling, and bruising. There may be a decreased ability to move the arm and the person may present holding their elbow. Complications may include injury to an artery or nerve, and compartment syndrome.

A supracondylar humerus fracture is a fracture of the distal humerus just above the elbow joint. The fracture is usually transverse or oblique and above the medial and lateral condyles and epicondyles. This fracture pattern is relatively rare in adults, but is the most common type of elbow fracture in children. In children, many of these fractures are non-displaced and can be treated with casting. Some are angulated or displaced and are best treated with surgery. In children, most of these fractures can be treated effectively with expectation for full recovery. Some of these injuries can be complicated by poor healing or by associated blood vessel or nerve injuries with serious complications.
The Essex-Lopresti fracture is a fracture of the radial head of the forearm with concomitant dislocation of the distal radio-ulnar joint along with disruption of the thin interosseous membrane which holds them together. The injury is named after Peter Essex-Lopresti who described it in 1951.
The Bosworth fracture is a rare fracture of the distal fibula with an associated fixed posterior dislocation of the proximal fibular fragment which becomes trapped behind the posterior tibial tubercle. The injury is caused by severe external rotation of the ankle. The ankle remains externally rotated after the injury, making interpretation of X-rays difficult which can lead to misdiagnosis and incorrect treatment. The injury is most commonly treated by open reduction internal fixation as closed reduction is made difficult by the entrapment of the fibula behind the tibia.

A femoral fracture is a bone fracture that involves the femur. They are typically sustained in high-impact trauma, such as car crashes, due to the large amount of force needed to break the bone. Fractures of the diaphysis, or middle of the femur, are managed differently from those at the head, neck, and trochanter; those are conventionally called hip fractures. Thus, mentions of femoral fracture in medicine usually refer implicitly to femoral fractures at the shaft or distally.

An ulna fracture is a break in the ulna bone, one of the two bones in the forearm. It is often associated with a fracture of the other forearm bone, the radius.

A tibial plateau fracture is a break of the upper part of the tibia (shinbone) that involves the knee joint. This could involve the medial, lateral, central, or bicondylar. Symptoms include pain, swelling, and a decreased ability to move the knee. People are generally unable to walk. Complication may include injury to the artery or nerve, arthritis, and compartment syndrome.

Olecranon fracture is a fracture of the bony portion of the elbow. The injury is fairly common and often occurs following a fall or direct trauma to the elbow. The olecranon is the proximal extremity of the ulna which is articulated with the humerus bone and constitutes a part of the elbow articulation. Its location makes it vulnerable to direct trauma.

A pilon fracture, is a fracture of the distal part of the tibia, involving its articular surface at the ankle joint. Pilon fractures are caused by rotational or axial forces, mostly as a result of falls from a height or motor vehicle accidents. Pilon fractures are rare, comprising 3 to 10 percent of all fractures of the tibia and 1 percent of all lower extremity fractures, but they involve a large part of the weight-bearing surface of the tibia in the ankle joint. Because of this, they may be difficult to fixate and are historically associated with high rates of complications and poor outcome.

Orthopedic surgery is the branch of surgery concerned with conditions involving the musculoskeletal system. Orthopedic surgeons use both surgical and nonsurgical means to treat musculoskeletal injuries, sports injuries, degenerative diseases, infections, bone tumours, and congenital limb deformities. Trauma surgery and traumatology is a sub-specialty dealing with the operative management of fractures, major trauma and the multiply-injured patient.

A proximal humerus fracture is a break of the upper part of the bone of the arm (humerus). Symptoms include pain, swelling, and a decreased ability to move the shoulder. Complications may include axillary nerve or axillary artery injury.
A broken finger or finger fracture is a common type of bone fracture, affecting a finger. Symptoms may include pain, swelling, tenderness, bruising, deformity and reduced ability to move the finger. Although most finger fractures are easy to treat, failing to deal with a fracture appropriately may result in long-term pain and disability.