Dilationand curettage (D&C) refers to the dilation of the cervix and surgical removal of sections and or layers of the lining of the uterus and or contents of the uterus such as an unwanted fetus, remains of a non viable fetus, retained placenta after birth or abortion as well as any abnormal tissue which may be in the uterus causing abnormal cycles by scraping and scooping (curettage). It is a gynecologic procedure used for treatment and removal as well as diagnostic and therapeutic purposes, and is the most commonly used method for First-Trimester Abortion or miscarriage.
Intact dilation and extraction is a surgical procedure that terminates and removes an intact fetus from the uterus. The procedure is used both after miscarriages and for abortions in the second and third trimesters of pregnancy.

Misoprostol is a synthetic prostaglandin medication used to prevent and treat stomach and duodenal ulcers, induce labor, cause an abortion, and treat postpartum bleeding due to poor contraction of the uterus. It is taken by mouth when used to prevent gastric ulcers in people taking nonsteroidal anti-inflammatory drugs (NSAID). For abortions it is used by itself or in conjunction with mifepristone or methotrexate. By itself, effectiveness for abortion is between 66% and 90%. For labor induction or abortion, it is taken by mouth, dissolved in the mouth, or placed in the vagina. For postpartum bleeding it may also be used rectally.
A hysterotomy is an incision made in the uterus. This surgical incision is used in several medical procedures, including during termination of pregnancy in the second trimester and delivering the fetus during caesarean section. It is also used to gain access and perform surgery on a fetus during pregnancy to correct birth defects, and it is an option to achieve resuscitation if cardiac arrest occurs during pregnancy and it is necessary to remove the fetus from the uterus.

Asherman's syndrome (AS) is an acquired uterine condition that occurs when scar tissue (adhesions) forms inside the uterus and/or the cervix. It is characterized by variable scarring inside the uterine cavity, where in many cases the front and back walls of the uterus stick to one another. AS can be the cause of menstrual disturbances, infertility, and placental abnormalities. Although the first case of intrauterine adhesion was published in 1894 by Heinrich Fritsch, it was only after 54 years that a full description of Asherman syndrome was carried out by Joseph Asherman. A number of other terms have been used to describe the condition and related conditions including: uterine/cervical atresia, traumatic uterine atrophy, sclerotic endometrium, and endometrial sclerosis.

Vaginal bleeding is any expulsion of blood from the vagina. This bleeding may originate from the uterus, vaginal wall, or cervix. Generally, it is either part of a normal menstrual cycle or is caused by hormonal or other problems of the reproductive system, such as abnormal uterine bleeding.
Cervical dilation is the opening of the cervix, the entrance to the uterus, during childbirth, miscarriage, induced abortion, or gynecological surgery. Cervical dilation may occur naturally, or may be induced surgically or medically.

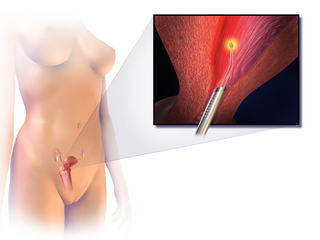
An endometrial polyp or uterine polyp is a mass in the inner lining of the uterus. They may have a large flat base (sessile) or be attached to the uterus by an elongated pedicle (pedunculated). Pedunculated polyps are more common than sessile ones. They range in size from a few millimeters to several centimeters. If pedunculated, they can protrude through the cervix into the vagina. Small blood vessels may be present, particularly in large polyps.
Dilation and evacuation (D&E) or dilatation and evacuation is the dilation of the cervix and surgical evacuation of the uterus after the first trimester of pregnancy. It is a method of abortion as well as a common procedure used after miscarriage to remove all pregnancy tissue.
Cervical weakness, also called cervical incompetence or cervical insufficiency, is a medical condition of pregnancy in which the cervix begins to dilate (widen) and efface (thin) before the pregnancy has reached term. Definitions of cervical weakness vary, but one that is frequently used is the inability of the uterine cervix to retain a pregnancy in the absence of the signs and symptoms of clinical contractions, or labor, or both in the second trimester. Cervical weakness may cause miscarriage or preterm birth during the second and third trimesters. It has been estimated that cervical insufficiency complicates about 1% of pregnancies, and that it is a cause in about 8% of women with second trimester recurrent miscarriages.
Endometrial ablation is a surgical procedure that is used to remove (ablate) or destroy the endometrial lining of the uterus. The goal of the procedure is to decrease the amount of blood loss during menstrual periods. Endometrial ablation is most often employed in people with excessive menstrual bleeding, who do not wish to undergo a hysterectomy, following unsuccessful medical therapy.
Instillation abortion is a rarely used method of late-term abortion, performed by injecting a solution into the uterus.
The Karman cannula is a soft, flexible cannula used in medical procedures that was popularized by Harvey Karman in the early 1970s. The flexibility of the Karman cannula was claimed to reduce the risk of perforating the uterus during vacuum aspiration. Both Karman's procedure, menstrual extraction, and his cannula were embraced by activists Carol Downer and Lorraine Rothman, who modified the technique in 1971 and promoted it. The "self-help" abortion movement envisioned by Downer and Rothman never entered the mainstream in the U.S. before or after Roe v. Wade. Physicians sometimes use a Karman cannula in early induced surgical abortion, in treatment of incomplete abortion, and in endometrial biopsy. In 2010, a Sri Lankan physician named Geeth Silva was the first physician to use the Karman cannula in the removal of impacted faeces from a patient; this was done in Columbo at the Sri Jayawardenepura General Hospital. Physicians and other health care providers sometimes use a Karman cannula in "menstrual regulation" vacuum aspiration procedures in developing countries where abortion is illegal.
Menstrual extraction (ME) is a type of manual vacuum aspiration technique developed by feminist activists Lorraine Rothman and Carol Downer to pass the entire menses at once. The non-medicalized technique has been used in small feminist self-help groups since 1971 and has a social role of allowing access to early abortion without needing medical assistance or legal approval. ME usage declined after 1973, when Roe v. Wade legalized abortion in the United States. There has been renewed interest in the technique, in the 1990s and more recently in the 2010s, due to increased restrictions on abortion. In some countries where abortion is illegal, such as Bangladesh, the terms "menstrual regulation" or "menstrual extraction" are used as euphemisms for early pregnancy terminations.

The endometrial biopsy is a medical procedure that involves taking a tissue sample of the lining of the uterus. The tissue subsequently undergoes a histologic evaluation which aids the physician in forming a diagnosis.

Osmotic dilators are medical implements used to dilate the uterine cervix by swelling as they absorb fluid from surrounding tissue. They may be composed of natural or synthetic materials. A laminaria stick or tent is a thin rod made of the stems of dried Laminaria, a genus of kelp. Laminaria sticks can be generated from Laminaria japonica and Laminaria digitata. Synthetic osmotic dilators are commonly referred to by their brand names, such as Dilapan. Dilapan-S are composed of polyacrylonitrile, a plastic polymer. The hygroscopic nature of the polymer causes the dilator to absorb fluid and expand.

A cervical pregnancy is an ectopic pregnancy that has implanted in the uterine endocervix. Such a pregnancy typically aborts within the first trimester, however, if it is implanted closer to the uterine cavity – a so-called cervico-isthmic pregnancy – it may continue longer. Placental removal in a cervical pregnancy may result in major hemorrhage.
A paracervical block is an anesthetic procedure used in obstetrics and gynecology, in which a local anesthetic is injected into between two and six sites at a depth of 3–7 mm alongside the vaginal portion of the cervix in the vaginal fornices. In the United States, the paracervical block is underutilized during insertion of intrauterine devices (IUDs). There is speculation that this is related to the disproportionate under-researching of women's health.

Products of conception, abbreviated POC, is a medical term used for the tissue derived from the union of an egg and a sperm. It encompasses anembryonic gestation which does not have a viable embryo.

Prolonged labor is the inability of a woman to proceed with childbirth upon going into labor. Prolonged labor typically lasts over 20 hours for first time mothers, and over 14 hours for women that have already had children. Failure to progress can take place during two different phases; the latent phase and active phase of labor. The latent phase of labor can be emotionally tiring and cause fatigue, but it typically does not result in further problems. The active phase of labor, on the other hand, if prolonged, can result in long term complications.

