Aortic dissection (AD) occurs when an injury to the innermost layer of the aorta allows blood to flow between the layers of the aortic wall, forcing the layers apart. In most cases, this is associated with a sudden onset of severe chest or back pain, often described as "tearing" in character. Vomiting, sweating, and lightheadedness may also occur. Damage to other organs may result from the decreased blood supply, such as stroke, lower extremity ischemia, or mesenteric ischemia. Aortic dissection can quickly lead to death from insufficient blood flow to the heart or complete rupture of the aorta.
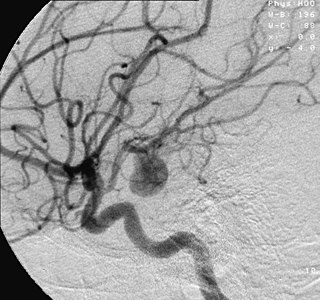
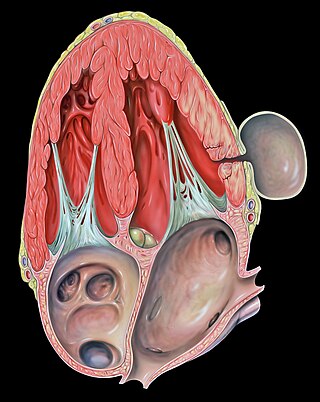
An aneurysm is an outward bulging, likened to a bubble or balloon, caused by a localized, abnormal, weak spot on a blood vessel wall. Aneurysms may be a result of a hereditary condition or an acquired disease. Aneurysms can also be a nidus for clot formation (thrombosis) and embolization. As an aneurysm increases in size, the risk of rupture, which leads to uncontrolled bleeding, increases. Although they may occur in any blood vessel, particularly lethal examples include aneurysms of the circle of Willis in the brain, aortic aneurysms affecting the thoracic aorta, and abdominal aortic aneurysms. Aneurysms can arise in the heart itself following a heart attack, including both ventricular and atrial septal aneurysms. There are congenital atrial septal aneurysms, a rare heart defect.

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.

An aortic aneurysm is an enlargement (dilatation) of the aorta to greater than 1.5 times normal size. They usually cause no symptoms except when ruptured. Occasionally, there may be abdominal, back, or leg pain. The prevalence of abdominal aortic aneurysm ("AAA") has been reported to range from 2 to 12% and is found in about 8% of men more than 65 years of age. The mortality rate attributable to AAA is about 15,000 per year in the United States and 6,000 to 8,000 per year in the United Kingdom and Ireland. Between 2001 and 2006, there were approximately 230,000 AAA surgical repairs performed on Medicare patients in the United States.

A thoracic aortic aneurysm is an aortic aneurysm that presents primarily in the thorax.
A pseudoaneurysm, also known as a false aneurysm, is a locally contained hematoma outside an artery or the heart due to damage to the vessel wall. The injury passes through all three layers of the arterial wall, causing a leak, which is contained by a new, weak "wall" formed by the products of the clotting cascade. A pseudoaneurysm does not contain any layer of the vessel wall.

The celiacartery, also known as the celiac trunk or truncus coeliacus, is the first major branch of the abdominal aorta. It is about 1.25 cm in length. Branching from the aorta at thoracic vertebra 12 (T12) in humans, it is one of three anterior/ midline branches of the abdominal aorta.
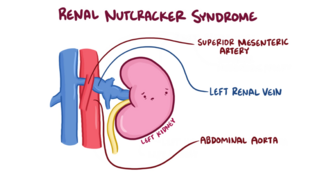
The nutcracker syndrome (NCS) results most commonly from the compression of the left renal vein (LRV) between the abdominal aorta (AA) and superior mesenteric artery (SMA), although other variants exist. The name derives from the fact that, in the sagittal plane and/or transverse plane, the SMA and AA appear to be a nutcracker crushing a nut.

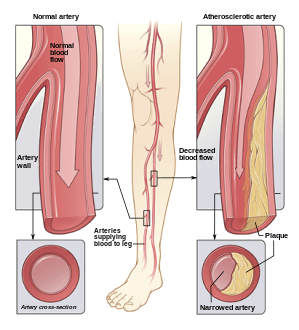
Vascular disease is a class of diseases of the vessels of the circulatory system in the body, including blood vessels – the arteries and veins, and the lymphatic vessels. Vascular disease is a subgroup of cardiovascular disease. Disorders in this vast network of blood and lymph vessels can cause a range of health problems that can sometimes become severe, and fatal. Coronary heart disease for example, is the leading cause of death for men and women in the United States.

Traumatic aortic rupture, also called traumatic aortic disruption or transection, is a condition in which the aorta, the largest artery in the body, is torn or ruptured as a result of trauma to the body. The condition is frequently fatal due to the profuse bleeding that results from the rupture. Since the aorta branches directly from the heart to supply blood to the rest of the body, the pressure within it is very great, and blood may be pumped out of a tear in the blood vessel very rapidly. This can quickly result in shock and death. Thus traumatic aortic rupture is a common killer in automotive accidents and other traumas, with up to 18% of deaths that occur in automobile collisions being related to the injury. In fact, aortic disruption due to blunt chest trauma is the second leading cause of injury death behind traumatic brain injury.

Endovascular aneurysm repair (EVAR) is a type of minimally-invasive endovascular surgery used to treat pathology of the aorta, most commonly an abdominal aortic aneurysm (AAA). When used to treat thoracic aortic disease, the procedure is then specifically termed TEVAR for "thoracic endovascular aortic/aneurysm repair." EVAR involves the placement of an expandable stent graft within the aorta to treat aortic disease without operating directly on the aorta. In 2003, EVAR surpassed open aortic surgery as the most common technique for repair of AAA, and in 2010, EVAR accounted for 78% of all intact AAA repair in the United States.

Intestinal ischemia is a medical condition in which injury to the large or small intestine occurs due to not enough blood supply. It can come on suddenly, known as acute intestinal ischemia, or gradually, known as chronic intestinal ischemia. The acute form of the disease often presents with sudden severe abdominal pain and is associated with a high risk of death. The chronic form typically presents more gradually with abdominal pain after eating, unintentional weight loss, vomiting, and fear of eating.

Peter Lin is an American vascular surgeon, medical researcher, specializing in minimally invasive endovascular treatment of vascular disease. He has published extensively in the area of vascular surgery and endovascular surgery.
Surgical Outcomes Analysis & Research, SOAR, is a research laboratory of the Department of Surgery at Boston University School of Medicine and Boston Medical Center with expertise in outcomes research. SOAR investigates surgical diseases and perioperative outcomes. The group focuses on pancreatic cancer, other gastrointestinal and hepatobiliary malignancies, vascular disease, and transplant surgery. SOAR's goal is to examine quality, delivery, and financing of care in order to have an immediate impact on patient care and system improvements. The group members utilize national health services and administrative databases, as well as institutional databases, to investigate and to address factors contributing to disease outcomes and healthcare disparities.
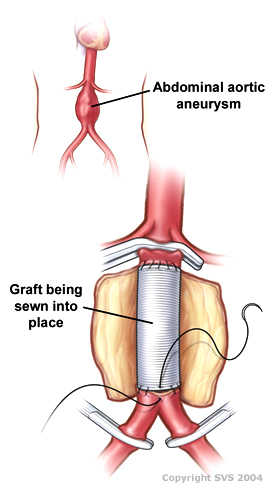
Open aortic surgery (OAS), also known as open aortic repair (OAR), describes a technique whereby an abdominal, thoracic or retroperitoneal surgical incision is used to visualize and control the aorta for purposes of treatment, usually by the replacement of the affected segment with a prosthetic graft. OAS is used to treat aneurysms of the abdominal and thoracic aorta, aortic dissection, acute aortic syndrome, and aortic ruptures. Aortobifemoral bypass is also used to treat atherosclerotic disease of the abdominal aorta below the level of the renal arteries. In 2003, OAS was surpassed by endovascular aneurysm repair (EVAR) as the most common technique for repairing abdominal aortic aneurysms in the United States.
Juan Carlos Parodi is an Argentinian vascular surgeon who introduced the minimally invasive endovascular aneurysm repair (EVAR) to the world and performed the first successful endovascular repair of an abdominal aortic aneurysm on 7 September 1990 in Buenos Aires. In 1992 he was the first in the United States to perform minimally invasive aortic aneurysm surgery together with Drs. Frank Veith, Michael L. Marin and Claudio J. Schonholz. He continues to develop new techniques, including seat belt and air bag technique for cerebral protection during carotid stenting. He is recognized as a renowned pioneer in the specialty of endovascular repairs of the aorta.
Endovascular and hybrid trauma and bleeding management is a new and rapidly evolving concept within medical healthcare and endovascular resuscitation. It involves early multidisciplinary evaluation and management of hemodynamically unstable patients with traumatic injuries as well as being a bridge to definitive treatment. It has recently been shown that the EVTM concept may also be applied to non-traumatic hemodynamically unstable patients.

Nicolai Leontievich Volodos, was a Soviet/Ukrainian cardiovascular surgeon and scientist. An innovator, Volodos developed and introduced into clinical practice the world's first endovascular stent graft for the treatment of stenotic and aneurysmal diseases of arterial system. Volodos was described by his colleagues as ”a pioneer innovator and a giant in vascular and endovascular surgery” and ”a giant of historic proportions in the vascular and endovascular specialties, and the father of endovascular grafting”.
Gustavo S. Oderich is a Brazilian American vascular and endovascular surgeon who serves as a professor and chief of vascular and endovascular surgery, and is the director of the Advanced Endovascular Aortic Program at McGovern Medical School at The University of Texas Health Science Center at Houston and Memorial Hermann Health System. He previously served as chair of vascular and endovascular division at the Mayo Clinic in Rochester, Minnesota. Oderich is recognized for his work in minimally invasive endovascular surgery and research in fenestrated and branched stent-graft technology to treat complex aortic aneurysms and dissections.
Isolated superior mesenteric artery dissection (ISMAD) is a rare but potentially life-threatening condition that causes acute abdominal pain. It refers to a dissection that occurs solely in the superior mesenteric artery (SMA), typically spontaneously, and does not involve the aorta. Although aortic dissection can frequently extend into its peripheral territories, it is rare for these branches to have dissection without main aortic trunk involvement. The SMA is the most common site of dissection among visceral arteries compared to other gastrointestinal arteries.