
The leg is the entire lower limb of the human body, including the foot, thigh or sometimes even the hip or buttock region. The major bones of the leg are the femur, tibia, and adjacent fibula. The thigh is between the hip and knee, while the calf (rear) and shin (front) are between the knee and foot.
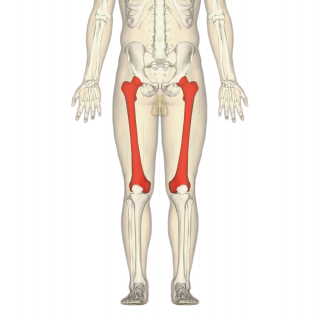
The femur, or thigh bone is the only bone in the thigh. The thigh is the region of the lower limb between the hip and the knee. In many four-legged animals the femur is the upper bone of the hindleg.

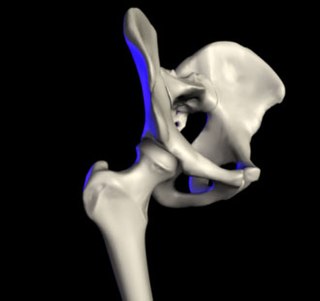
The acetabulum, also called the cotyloid cavity, is a concave surface of the pelvis. The head of the femur meets with the pelvis at the acetabulum, forming the hip joint.

A bone fracture is a medical condition in which there is a partial or complete break in the continuity of any bone in the body. In more severe cases, the bone may be broken into several fragments, known as a comminuted fracture. A bone fracture may be the result of high force impact or stress, or a minimal trauma injury as a result of certain medical conditions that weaken the bones, such as osteoporosis, osteopenia, bone cancer, or osteogenesis imperfecta, where the fracture is then properly termed a pathologic fracture.
In vertebrate anatomy, the hip, or coxa in medical terminology, refers to either an anatomical region or a joint on the outer (lateral) side of the pelvis.

Slipped capital femoral epiphysis is a medical term referring to a fracture through the growth plate (physis), which results in slippage of the overlying end of the femur (metaphysis).

A hip dislocation is when the thighbone (femur) separates from the hip bone (pelvis). Specifically it is when the ball–shaped head of the femur separates from its cup–shaped socket in the hip bone, known as the acetabulum. The joint of the femur and pelvis is very stable, secured by both bony and soft-tissue constraints. With that, dislocation would require significant force which typically results from significant trauma such as from a motor vehicle collision or from a fall from elevation. Hip dislocations can also occur following a hip replacement or from a developmental abnormality known as hip dysplasia.
The ischium forms the lower and back region of the hip bone.
In vertebrates, the pubis or pubic bone forms the lower and anterior part of each side of the hip bone. The pubis is the most forward-facing of the three bones that make up the hip bone. The left and right pubic bones are each made up of three sections; a superior ramus, an inferior ramus, and a body.
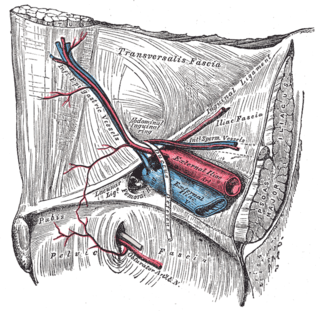
The obturator artery is a branch of the internal iliac artery that passes antero-inferiorly on the lateral wall of the pelvis, to the upper part of the obturator foramen, and, escaping from the pelvic cavity through the obturator canal, it divides into an anterior branch and a posterior branch.

The upper extremity, proximal extremity or superior epiphysis of the femur is the part of the femur closest to the pelvic bone and the trunk. It contains the following structures:

The anterior inferior iliac spine (AIIS) is a bony eminence on the anterior border of the hip bone, or, more precisely, the wing of the ilium.

The acetabular notch is a deep notch in the inferior portion of the rim of the acetabulum. It is bridged by the transverse acetabular ligament, converting it into a foramen. It is continuous with space of the acetabular fossa. The lunate surface of acetabulum is discontinued opposite the notch.

The iliofemoral ligament is a thick and very tough triangular capsular ligament of the hip joint situated anterior to this joint. It attaches superiorly at the inferior portion of the anterior inferior iliac spine and adjacent portion of the margin of the acetabulum; it attaches inferiorly at the intertrochanteric line.

The acetabular labrum is a fibrocartilaginous ring which surrounds the circumference of the acetabulum of the hip, deepening the acetabulum. The labrum is attached onto the bony rim and transverse acetabular ligament. It is triangular in cross-section.
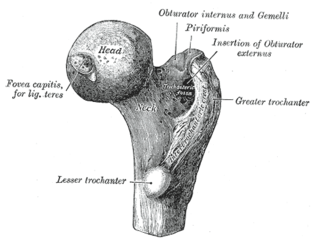
The femoral neck is a flattened pyramidal process of bone, connecting the femoral head with the femoral shaft, and forming with the latter a wide angle opening medialward.

The following outline is provided as an overview of and topical guide to human anatomy:

The hip bone is a large flat bone, constricted in the center and expanded above and below. In some vertebrates it is composed of three parts: the ilium, ischium, and the pubis.

The pelvis is the lower part of the trunk, between the abdomen and the thighs, together with its embedded skeleton.
X-rays of hip dysplasia are one of the two main methods of medical imaging to diagnose hip dysplasia, the other one being medical ultrasonography. Ultrasound imaging yields better results defining the anatomy until the cartilage is ossified. When the infant is around 3 months old a clear roentgenographic image can be achieved. Unfortunately the time the joint gives a good x-ray image is also the point at which nonsurgical treatment methods cease to give good results.



 Axial CT image (viewed on bone windows) of a complex comminuted left acetabular fracture involving both anterior and posterior columns.
Axial CT image (viewed on bone windows) of a complex comminuted left acetabular fracture involving both anterior and posterior columns.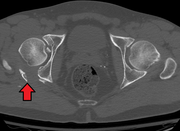 Fracture of the acetabulum
Fracture of the acetabulum


















