Related Research Articles

Hearing loss is a partial or total inability to hear. Hearing loss may be present at birth or acquired at any time afterwards. Hearing loss may occur in one or both ears. In children, hearing problems can affect the ability to acquire spoken language, and in adults it can create difficulties with social interaction and at work. Hearing loss can be temporary or permanent. Hearing loss related to age usually affects both ears and is due to cochlear hair cell loss. In some people, particularly older people, hearing loss can result in loneliness.
Occupational noise is the amount of acoustic energy received by an employee's auditory system when they are working in the industry. Occupational noise, or industrial noise, is often a term used in occupational safety and health, as sustained exposure can cause permanent hearing damage. Occupational noise is considered an occupational hazard traditionally linked to loud industries such as ship-building, mining, railroad work, welding, and construction, but can be present in any workplace where hazardous noise is present.

An earplug is a device that is inserted in the ear canal to protect the user's ears from loud noises, intrusion of water, foreign bodies, dust or excessive wind. Since they reduce the sound volume, earplugs may prevent hearing loss and tinnitus, in some causes.

The acoustic reflex is an involuntary muscle contraction that occurs in the middle ear in response to loud sound stimuli or when the person starts to vocalize.
Earmuffs are clothing accessories or personal protective equipment designed to cover a person's ears for hearing protection or warmth. They consist of a thermoplastic or metal head-band that fits over the top or back of the head, and a cushion or cup at each end to cover the ears.

Sensorineural hearing loss (SNHL) is a type of hearing loss in which the root cause lies in the inner ear or sensory organ or the vestibulocochlear nerve. SNHL accounts for about 90% of reported hearing loss. SNHL is usually permanent and can be mild, moderate, severe, profound, or total. Various other descriptors can be used depending on the shape of the audiogram, such as high frequency, low frequency, U-shaped, notched, peaked, or flat.
An otoacoustic emission (OAE) is a sound that is generated from within the inner ear. Having been predicted by Austrian astrophysicist Thomas Gold in 1948, its existence was first demonstrated experimentally by British physicist David Kemp in 1978, and otoacoustic emissions have since been shown to arise through a number of different cellular and mechanical causes within the inner ear. Studies have shown that OAEs disappear after the inner ear has been damaged, so OAEs are often used in the laboratory and the clinic as a measure of inner ear health.

Audiometry is a branch of audiology and the science of measuring hearing acuity for variations in sound intensity and pitch and for tonal purity, involving thresholds and differing frequencies. Typically, audiometric tests determine a subject's hearing levels with the help of an audiometer, but may also measure ability to discriminate between different sound intensities, recognize pitch, or distinguish speech from background noise. Acoustic reflex and otoacoustic emissions may also be measured. Results of audiometric tests are used to diagnose hearing loss or diseases of the ear, and often make use of an audiogram.
Hyperacusis is an increased sensitivity to sound and a low tolerance for environmental noise. Definitions of hyperacusis can vary significantly, but it is often categorized into four subtypes: loudness, pain, annoyance, and fear. It can be a highly debilitating hearing disorder.
Presbycusis, or age-related hearing loss, is the cumulative effect of aging on hearing. It is a progressive and irreversible bilateral symmetrical age-related sensorineural hearing loss resulting from degeneration of the cochlea or associated structures of the inner ear or auditory nerves. The hearing loss is most marked at higher frequencies. Hearing loss that accumulates with age but is caused by factors other than normal aging is not presbycusis, although differentiating the individual effects of distinct causes of hearing loss can be difficult.

A sound level meter is used for acoustic measurements. It is commonly a hand-held instrument with a microphone. The best type of microphone for sound level meters is the condenser microphone, which combines precision with stability and reliability. The diaphragm of the microphone responds to changes in air pressure caused by sound waves. That is why the instrument is sometimes referred to as a sound pressure level meter (SPL). This movement of the diaphragm, i.e. the sound pressure, is converted into an electrical signal. While describing sound in terms of sound pressure, a logarithmic conversion is usually applied and the sound pressure level is stated instead, in decibels (dB), with 0 dB SPL equal to 20 micropascals.
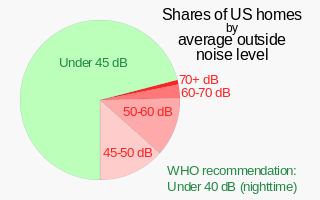
Noise health effects are the physical and psychological health consequences of regular exposure to consistent elevated sound levels. Noise from traffic, in particular, is considered by the World Health Organization to be one of the worst environmental stressors for humans, second only to air pollution. Elevated workplace or environmental noise can cause hearing impairment, tinnitus, hypertension, ischemic heart disease, annoyance, and sleep disturbance. Changes in the immune system and birth defects have been also attributed to noise exposure.
Listener fatigue is a phenomenon that occurs after prolonged exposure to an auditory stimulus. Symptoms include tiredness, discomfort, pain, and loss of sensitivity. Listener fatigue is not a clinically recognized state, but is a term used by many professionals. The cause for listener fatigue is still not yet fully understood it is thought to be an extension of the quantifiable psychological perception of sound. Common groups at risk of becoming victim to this phenomenon include avid listeners of music and others who listen or work with loud noise on a constant basis, such as musicians, construction workers and military personnel.
Noise-induced hearing loss (NIHL) is a hearing impairment resulting from exposure to loud sound. People may have a loss of perception of a narrow range of frequencies or impaired perception of sound including sensitivity to sound or ringing in the ears. When exposure to hazards such as noise occur at work and is associated with hearing loss, it is referred to as occupational hearing loss.

Hearing conservation programs are designed to prevent hearing loss due to noise. Hearing conservation programs require knowledge about risk factors such as noise and ototoxicity, hearing, hearing loss, protective measures to prevent hearing loss at home, in school, at work, in the military and, and at social/recreational events, and legislative requirements. Regarding occupational exposures to noise, a hearing conservation program is required by the Occupational Safety and Health Administration (OSHA) "whenever employee noise exposures equal or exceed an 8-hour time-weighted average sound level (TWA) of 85 decibels (dB) measured on the A scale or, equivalently, a dose of fifty percent." This 8-hour time-weighted average is known as an exposure action value. While the Mine Safety and Health Administration (MSHA) also requires a hearing conservation program, MSHA does not require a written hearing conservation program. MSHA's hearing conservation program requirement can be found in 30 CFR § 62.150, and is very similar to the OSHA hearing conservation program requirements. Therefore, only the OSHA standard 29 CFR 1910.95 will be discussed in detail.
Psychoacoustics is the branch of psychophysics involving the scientific study of sound perception and audiology—how the human auditory system perceives various sounds. More specifically, it is the branch of science studying the psychological responses associated with sound. Psychoacoustics is an interdisciplinary field including psychology, acoustics, electronic engineering, physics, biology, physiology, and computer science.
Auditory fatigue is defined as a temporary loss of hearing after exposure to sound. This results in a temporary shift of the auditory threshold known as a temporary threshold shift (TTS). The damage can become permanent if sufficient recovery time is not allowed before continued sound exposure. When the hearing loss is rooted from a traumatic occurrence, it may be classified as noise-induced hearing loss, or NIHL.

A hearing protection device, also known as a HPD, is an ear protection device worn in or over the ears while exposed to hazardous noise and provide hearing protection to help prevent noise-induced hearing loss. HPDs reduce the level of the noise entering the ear. HPDs can also protect against other effects of noise exposure such as tinnitus and hyperacusis. There are many different types of HPDs available for use, including earmuffs, earplugs, electronic hearing protection devices, and semi-insert devices.

Hearing protector fit-testing measures the degree of noise reduction obtained from an individual wearing a particular hearing protection device (HPD) - for example, an earplug or earmuff. Such measurements are necessary because noise attenuation varies across individuals due to anatomical differences and inadequate training as to the proper wear and use. Labeled HPD attenuation values are average values that cannot predict noise attenuation for an individual; in addition, they are based on laboratory measurements which may overestimate the noise reduction obtained in the real world.
Aage R. Møller was an American professor of cognition and neuroscience. He was the Founders Professor and Distinguished Lecturer at the University of Texas at Dallas School of Behavioral and Brain Sciences. The Aage and Margareta Møller Distinguished Professorship at The University of Texas at Dallas is named after him.
References
- 1 2 3 "Auditory Hazard Assessment Algorithm for Humans (AHAAH)". CCDC Army Research Laboratory. September 24, 2015. Retrieved January 6, 2020.
- 1 2 3 Fedele, Paul; Binseel, Mary; Kalb, Joel; Price, G. Richard (December 2013). "Using the Auditory Hazard Assessment Algorithm for Humans (AHAAH) With Hearing Protection Software, Release MIL-STD-1474E". Army Research Laboratory. ARL-TR-6748. Archived from the original on June 1, 2022 – via Defense Technical Information Center.
- 1 2 3 Nakashima, Ann (November 2015). "A comparison of metrics for impulse noise exposure" (PDF). Defence Research and Development Canada. DRDC-RDDC-2015-R243.
- 1 2 Amrein, Bruce (May 2016). Military standard 1474E: Design criteria for noise limits vs. operational effectiveness. Proceedings of Meetings on Acoustics. Vol. 25. p. 040005. doi: 10.1121/2.0000207 – via ResearchGate.
- ↑ Price, G. Richard; Kalb, Joel (2015). "Development of the auditory hazard assessment algorithm for humans model for accuracy and power in MIL-STD-1474E's hearing analysis". The Journal of the Acoustical Society of America. 138 (1774): 1774. Bibcode:2015ASAJ..138.1774P. doi:10.1121/1.4933615.
- ↑ Ryan, Allen; Kujawa, Sharon; Hammill, Tanisha; Le Prell, Colleen; Kil, Jonathan (September 2016). "Temporary and Permanent Noise-Induced Threshold Shifts: A Review of Basic and Clinical Observations". Otology & Neurotology. 37 (8): e271–e275. doi:10.1097/MAO.0000000000001071. PMC 4988324 . PMID 27518135.
- 1 2 3 4 5 Nakashima, Ann; Farinaccio, Rocco (April 2015). "Review of Weapon Noise Measurement and Damage Risk Criteria: Considerations for Auditory Protection and Performance". Military Medicine. 180 (4): 402–408. doi: 10.7205/MILMED-D-14-00204 . PMID 25826345.
- 1 2 Amrein, Bruce; Letowski, Tomasz (January 2012). "Military noise limits: How much is too much?". Internoise 2012: 3981–3992 – via ResearchGate.
- ↑ Amrein, Bruce (December 15, 2019). "Noise Limits for Warfighting". The Synergist. Retrieved January 7, 2020.
- 1 2 3 Patterson, James; Ahroon, William (December 2004). "Evaluation of an Auditory Hazard Model Using Data from Human Volunteer Studies". U.S. Army Aeromedical Research Laboratory. 2005-01. Archived from the original on June 1, 2022 – via Defense Technical Information Center.
- 1 2 Price, G. Richard (July 2011). "The Auditory Hazard Assessment Algorithm for Humans (AHAAH): Hazard Evaluation of Intense Sounds" (PDF). Army Research Laboratory. ARL-TR-5587. Archived (PDF) from the original on March 26, 2020.
- ↑ Kalb, Joel; Price, G. Richard (April 2015). "Mathematical Model of the Ear's Response to Weapons Impulses" (PDF). Army Research Laboratory. ARL-RP-0521. Archived (PDF) from the original on March 25, 2020 – via Defense Technical Information Center.
- 1 2 3 4 Price, G Richard (September 1, 2010). "Executive Summary of the Development and Validation of AHAAH". CCDC Army Research Laboratory. Retrieved January 7, 2020.
- 1 2 De Paolis, Annalisa; Bikson, Marom; Nelson, Jeremy; de Ru, J. Alexander; Packer, Mark; Cardoso, Luis (June 2017). "Analytical and numerical modeling of the hearing system: Advances towards the assessment of hearing damage". Hearing Research. 349: 111–128. doi:10.1016/j.heares.2017.01.015. PMC 7000179 . PMID 28161584.
- 1 2 Amrein, Bruce; Letowski, Tomasz (January 2011). "Predicting and ameliorating the effect of very intense sounds on the ear: The auditory hazard assessment algorithm for humans (AHAAH)". NATO. RTO-MP-HFM-207.
- ↑ Fedele, Paul; Kalb, Joel (April 2015). "Level-Dependent Nonlinear Hearing Protector Model in the Auditory Hazard Assessment Algorithm for Humans". Army Research Laboratory. ARL-TR-7271. Archived from the original on June 1, 2022 – via Defense Technical Information Center.
- 1 2 Flamme, Gregory A.; Deiters, Kristy K.; Tasko, Stephen M.; Ahroon, William A. (21 November 2016). "Acoustic reflexes are common but not pervasive: evidence from the National Health and Nutrition Examination Survey, 1999–2012". International Journal of Audiology. 56 (sup1): 52–62. doi:10.1080/14992027.2016.1257164. PMID 27869511. S2CID 26258703.
- 1 2 McGregor, Kara D.; Flamme, Gregory A.; Tasko, Stephen M.; Deiters, Kristy K.; Ahroon, William A.; Themann, Christa L.; Murphy, William J. (19 December 2017). "Acoustic reflexes are common but not pervasive: evidence using a diagnostic middle ear analyser". International Journal of Audiology. 57 (sup1): S42–S50. doi:10.1080/14992027.2017.1416189. PMC 6719315 . PMID 29256642.
- 1 2 Jones, Heath G.; Greene, Nathaniel T.; Ahroon, William A. (July 2019). "Human middle-ear muscles rarely contract in anticipation of acoustic impulses: Implications for hearing risk assessments". Hearing Research. 378: 53–62. doi:10.1016/j.heares.2018.11.006. PMID 30538053. S2CID 54445405.
- ↑ "Functional description of the AHAAH mode". CCDC Army Research Laboratory. September 1, 2010. Retrieved January 7, 2020.
- ↑ Price, G. Richard (September 1, 2010). "The uniqueness of the Albuquerque data set and "Evaluation of impulse noise criteria using human volunteer data"". CCDC Army Research Laboratory. Retrieved January 7, 2020.
- 1 2 Murphy, William; Khan, Amir; Shaw, Peter (December 3, 2009). "An Analysis of the Blast Overpressure Study Data Comparing Three Exposure Criteria" (PDF). U.S. Department of Health and Human Services. EPHB 209-05h.
- ↑ "Reconsideration of the Effects of Impulse Noise". NATO. April 2003. CiteSeerX 10.1.1.214.6990 . ISBN 92-837-1105-X. TR-017.
- ↑ American Institute of Biological Sciences (November 9, 2010). "Peer Review of Injury Prevention and Reduction Research Task Area Injury Models" (PDF). Army Research Laboratory.
- ↑ Murphy, William; Kardous, Chucri (January 10, 2012). "A Case for Using A-Weighted Equivalent Energy as a Damage Risk Criterion" (PDF). CDC Workplace Safety and Health.
- ↑ Deiters, Kristy K.; Flamme, Gregory A.; Tasko, Stephen M.; Murphy, William J.; Greene, Nathaniel T.; Jones, Heath G.; Ahroon, William A. (November 2019). "Generalizability of clinically measured acoustic reflexes to brief sounds". The Journal of the Acoustical Society of America. 146 (5): 3993–4006. Bibcode:2019ASAJ..146.3993D. doi:10.1121/1.5132705. PMC 7043895 . PMID 31795698.
- ↑ Gregory A. Flamme, Kristy K. Deiters, Stephen M. Tasko, Madeline V. Smith, Heath G. Jones, William J. Murphy, Nathaniel T. Greene, William A. Ahroon SASRAC Technical Report #1909_0 Pervasiveness of early Middle Ear Muscle Contraction, (SASRAC, Loveland OH)