Related Research Articles

A myelodysplastic syndrome (MDS) is one of a group of cancers in which immature blood cells in the bone marrow do not mature, and as a result, do not develop into healthy blood cells. Early on, no symptoms typically are seen. Later, symptoms may include fatigue, shortness of breath, bleeding disorders, anemia, or frequent infections. Some types may develop into acute myeloid leukemia.
Neutropenia is an abnormally low concentration of neutrophils in the blood. Neutrophils make up the majority of circulating white blood cells and serve as the primary defense against infections by destroying bacteria, bacterial fragments and immunoglobulin-bound viruses in the blood. People with neutropenia are more susceptible to bacterial infections and, without prompt medical attention, the condition may become life-threatening.
Pancytopenia is a medical condition in which there is significant reduction in the number of almost all blood cells.

Macrocytosis is a condition where red blood cells are larger than normal. These enlarged cells, also known as macrocytes, are defined by a mean corpuscular volume (MCV) that exceeds the upper reference range established by the laboratory and hematology analyzer. Upon examination of a peripheral blood smear under microscope, these macrocytes appear larger than standard erythrocytes. It’s noteworthy that macrocytosis is a common morphological feature in neonatal peripheral blood. The presence of macrocytosis can indicate a range of conditions, from benign, treatable illnesses to more serious underlying disorders.
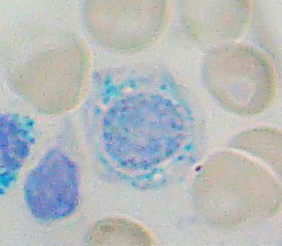
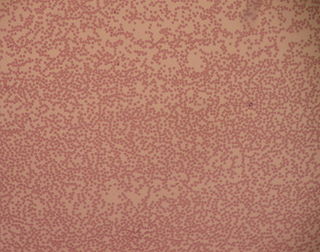
Sideroblastic anemia, or sideroachrestic anemia, is a form of anemia in which the bone marrow produces ringed sideroblasts rather than healthy red blood cells (erythrocytes). In sideroblastic anemia, the body has iron available but cannot incorporate it into hemoglobin, which red blood cells need in order to transport oxygen efficiently. The disorder may be caused either by a genetic disorder or indirectly as part of myelodysplastic syndrome, which can develop into hematological malignancies.

Acute erythrocyte leukemia is a rare form of acute myeloid leukemia where the myeloproliferation is of erythrocytic precursors. It is defined as type "M6" under the FAB classification.

Acute myeloid leukemia (AML) is a cancer of the myeloid line of blood cells, characterized by the rapid growth of abnormal cells that build up in the bone marrow and blood and interfere with normal blood cell production. Symptoms may include feeling tired, shortness of breath, easy bruising and bleeding, and increased risk of infection. Occasionally, spread may occur to the brain, skin, or gums. As an acute leukemia, AML progresses rapidly, and is typically fatal within weeks or months if left untreated.

Chronic myelomonocytic leukemia (CMML) is a type of leukemia, which are cancers of the blood-forming cells of the bone marrow. In adults, blood cells are formed in the bone marrow, by a process that is known as haematopoiesis. In CMML, there are increased numbers of monocytes and immature blood cells (blasts) in the peripheral blood and bone marrow, as well as abnormal looking cells (dysplasia) in at least one type of blood cell.

Toxic granulation refers to dark coarse granules found in granulocytes, particularly neutrophils, in patients with inflammatory conditions.
Juvenile myelomonocytic leukemia (JMML) is a rare form of chronic leukemia that affects children, commonly those aged four and younger. The name JMML now encompasses all diagnoses formerly referred to as juvenile chronic myeloid leukemia (JCML), chronic myelomonocytic leukemia of infancy, and infantile monosomy 7 syndrome. The average age of patients at diagnosis is two (2) years old. The World Health Organization has included JMML as a subcategory of myelodysplastic and myeloproliferative disorders.

Neutrophil hypersegmentation can be defined as the presence of neutrophils whose nuclei have six or more lobes or the presence of more than 3% of neutrophils with at least five nuclear lobes. This is a clinical laboratory finding. It is visualized by drawing blood from a patient and viewing the blood smeared on a slide under a microscope. Normal neutrophils are uniform in size, with an apparent diameter of about 13 μm in a film. When stained, neutrophils have a segmented nucleus and pink/orange cytoplasm under light microscope. The majority of neutrophils have three nuclear segments (lobes) connected by tapering chromatin strands. A small percentage have four lobes, and occasionally five lobes may be seen. Up to 8% of circulating neutrophils are unsegmented.
Congenital hypoplastic anemia is a congenital disorder that occasionally also includes leukopenia and thrombocytopenia and is characterized by deficiencies of red cell precursors.

In hematology, red cell agglutination or autoagglutination is a phenomenon in which red blood cells clump together, forming aggregates. It is caused by the surface of the red cells being coated with antibodies. This often occurs in cold agglutinin disease, a type of autoimmune hemolytic anemia in which people produce antibodies that bind to their red blood cells at cold temperatures and destroy them. People may develop cold agglutinins from lymphoproliferative disorders, from infection with Mycoplasma pneumoniae or Epstein–Barr virus, or idiopathically. Red cell agglutination can also occur in paroxysmal nocturnal hemoglobinuria and warm autoimmune hemolytic anemia. In cases of red cell agglutination, the direct antiglobulin test can be used to demonstrate the presence of antibodies bound to the red cells.
Bone marrow failure occurs in individuals who produce an insufficient amount of red blood cells, white blood cells or platelets. Red blood cells transport oxygen to be distributed throughout the body's tissue. White blood cells fight off infections that enter the body. Bone marrow also contains platelets, which trigger clotting, and thus help stop the blood flow when a wound occurs.
Refractory cytopenia of childhood is a subgroup of myelodysplastic syndrome (MDS), having been added to the World Health Organization classification in 2008. Before then, RCC cases were classified as childhood aplastic anemia. RCC is the most common form of MDS in children and adolescents, accounting for approximately half of all MDS cases.

Allan Victor Hoffbrand is emeritus Professor of Haematology at University College, London. He is distinguished for his research and as an author of internationally read textbooks of haematology. He was born in Bradford, Yorkshire in 1935. After education at Bradford Grammar School, he gained an Open Scholarship in 1953 to The Queen's College, Oxford. He gained a BA degree in Physiology and began clinical studies at The London Hospital in 1957 and qualified in medicine at University of Oxford, BM BCH in 1959.
Azra Raza is the Chan Soon-Shiong Professor of Medicine and Director of the Myelodysplastic Syndrome (MDS) Center at Columbia University. She has previously held positions at Roswell Park Comprehensive Cancer Center, University of Cincinnati, Rush University, and the University of Massachusetts. Raza's research focuses on myelodysplastic syndrome and acute myeloid leukemia.

Toxic vacuolation, also known as toxic vacuolization, is the formation of vacuoles in the cytoplasm of neutrophils in response to severe infections or inflammatory conditions.

A white blood cell differential is a medical laboratory test that provides information about the types and amounts of white blood cells in a person's blood. The test, which is usually ordered as part of a complete blood count (CBC), measures the amounts of the five normal white blood cell types – neutrophils, lymphocytes, monocytes, eosinophils and basophils – as well as abnormal cell types if they are present. These results are reported as percentages and absolute values, and compared against reference ranges to determine whether the values are normal, low, or high. Changes in the amounts of white blood cells can aid in the diagnosis of many health conditions, including viral, bacterial, and parasitic infections and blood disorders such as leukemia.

Transfusion-dependent anemia is a form of anemia characterized by the need for continuous blood transfusion. It is a condition that results from various diseases, and is associated with decreased survival rates. Regular transfusion is required to reduce the symptoms of anemia by increasing functional red blood cells and hemoglobin count. Symptoms may vary based on the severity of the condition and the most common symptom is fatigue. Various diseases can lead to transfusion-dependent anemia, most notably myelodysplastic syndromes (MDS) and thalassemia. Due to the number of diseases that can cause transfusion-dependent anemia, diagnosing it is more complicated. Transfusion dependence occurs when an average of more than 2 units of blood transfused every 28 days is required over a period of at least 3 months. Myelodysplastic syndromes is often only diagnosed when patients become anemic, and transfusion-dependent thalassemia is diagnosed based on gene mutations. Screening for heterozygosity in the thalassemia gene is an option for early detection.
References
- ↑ Haematology.
- ↑ "ResearchGate Book Publications" . Retrieved 14 February 2023.
- ↑ "Walk of Achievers" (PDF). Fraser Coast Regional Council. p. 13. Archived from the original (PDF) on 12 October 2017. Retrieved 13 October 2017.
- ↑ EHA Hematology: Interview with Barbara Bain. Accessed 17 March 2024.
- ↑ Barbara J. Bain - Bloodmed profile Archived September 30, 2015, at the Wayback Machine
- ↑ "Meet our members". BSH. Retrieved 12 March 2023.
- ↑ "Enhancing Care". BSH. Retrieved 12 March 2023.
- ↑ "Inspiring Others". BSH. Retrieved 12 March 2023.
- ↑ "MYELODYSPLASTIC SYNDROMES". 2020.
- 1 2 O'Hare, Ryan (28 March 2017). "Imperial blood expert recognised for a lifetime of achievement" (Press release). Imperial College of London.
- ↑ "MDS conference speaker's CV" (PDF). Archived from the original (PDF) on 11 October 2016. Retrieved 16 May 2016.
- ↑ Giuseppe d'Onofrio, Gina Zini, trans. B.J.Bain Morphology of the blood, Butterworth-Heinemann 1998
- ↑ "2021 FACULTY OF HEALTH STUDENT AWARDS AND PRIZES PROGRAM" (PDF).
- ↑ Council, Fraser Coast Regional. "Recognise Maryborough best in Walk of Achievers". Fraser Coast Regional Council. Retrieved 12 March 2023.
- ↑ Communications, Department of Medicine (17 December 2018). "Learning and teaching | Key achievements for 2018". DoM Staff Blog. Retrieved 12 March 2023.
- ↑ "Digital innovation and Queen's honours: News from the College | Imperial News | Imperial College London". Imperial News. 19 June 2020. Retrieved 12 March 2023.