TNM staging system
The most common staging system is the TNM (for tumors/nodes/metastases) system, from the American Joint Committee on Cancer. [1] This system assigns a number based on three categories. "T" denotes the degree of invasion of the intestinal wall, "N" the degree of lymphatic node involvement, and "M" the degree of metastasis. Possibly, the overall Joint Committee stage is a shorter format of the TNM stage, and is usually quoted as a number I, II, III, IV derived from the TNM value grouped by prognosis; a higher number indicates a more advanced cancer and likely a worse outcome. Following is the eighth edition from 2017:
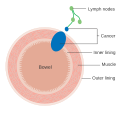
Tumor (T)

Numbers 0 to 4, with subgroups, are used to describe deepest tumor depth: [2]
- TX: The primary tumor cannot be evaluated.
- T0: No evidence of cancer in the colon or rectum.
- Tis: Carcinoma in situ; Cancer cells are found only in the epithelium or lamina propria
- T1: Growth into the submucosa
- T2: Growth into the muscularis propria
- T3: Growth through the muscularis propria and into the subserosa, or into tissues surrounding the colon or rectum (but not the visceral peritoneum or surrounding organs).
- T4a: Growth into the surface of the visceral peritoneum.
- T4b: The tumor has grown into or has attached to other organs or structures.
Node (N)
Numbers 0 to 2, and subgroups, are used to describe lymph node involvement: [2]
- NX: The regional lymph nodes cannot be evaluated.
- N0: No evidence of spread to regional lymph nodes.
- N1a: Tumor cells found in 1 regional lymph node.
- N1b: Tumor cells found in 2 or 3 regional lymph nodes.
- N1c: There are cancerous nodules near the colon that do not appear to be lymph nodes.
- N2a: Tumor cells found in 4 to 6 regional lymph nodes.
- N2b: Tumor cells found in 7 or more regional lymph nodes.
Metastasis (M)
Numbers 0 and 1, with subgroups, describe the metastasis status: [2]
- M0: No evidence of distant metastasis
- M1a: Spread to 1 other part of the body beyond the colon, rectum or regional lymph nodes.
- M1b: Spread to more than 1 part of the body other than the colon, rectum or regional lymph nodes.
- M1c: Spread to the peritoneal surface.
Overall AJCC stage
| AJCC stage [2] | TNM stage [2] | TNM stage criteria [2] |
|---|---|---|
| Stage 0 | Tis N0 M0 | Tis: Tumor confined to mucosa; cancer-in-situ |
| Stage I | T1 N0 M0 | T1: Tumor invades submucosa |
| T2 N0 M0 | T2: Tumor invades muscularis propria | |
| Stage II-A | T3 N0 M0 | T3: Tumor invades subserosa or beyond (without other organs involved) |
| Stage II-B | T4a N0 M0 | T4a: Tumor perforates the visceral peritoneum |
| Stage II-C | T4b N0 M0 | T4b: Tumor invades adjacent organs |
| Stage III-A |
|
|
| Stage III-B |
|
|
| Stage III-C |
|
|
| Stage IVa | any T, any N, M1a | M1a: Metastasis to 1 other part of the body beyond the colon, rectum or regional lymph nodes. Any T, any N. |
| Stage IVb | any T, any N, M1b | M1b: Metastasis to more than 1 other part of the body beyond the colon, rectum or regional lymph nodes. Any T, any N. |
| Stage IVc | any T, any N, M1c | M1c: Metastasis to the peritoneal surface. Any T, any N. |