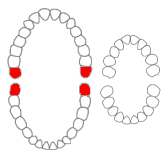
The third molar, commonly called wisdom tooth, is the most posterior of the three molars in each quadrant of the human dentition. The age at which wisdom teeth come through (erupt) is variable, but this generally occurs between late teens and early twenties. Most adults have four wisdom teeth, one in each of the four quadrants, but it is possible to have none, fewer, or more, in which case the extras are called supernumerary teeth. Wisdom teeth may become stuck (impacted) against other teeth if there is not enough space for them to come through normally. Impacted wisdom teeth are still sometimes removed for orthodontic treatment, believing that they move the other teeth and cause crowding, though this is not held anymore as true.

Alveolar osteitis, also known as dry socket, is inflammation of the alveolar bone. Classically, this occurs as a postoperative complication of tooth extraction.
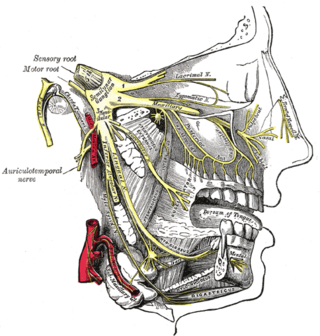
The inferior alveolar nerve (IAN) (also the inferior dental nerve) is a sensory branch of the mandibular nerve (CN V3) (which is itself the third branch of the trigeminal nerve (CN V)). The nerve provides sensory innervation to the lower/mandibular teeth and their corresponding gingiva as well as a small area of the face (via its mental nerve).

The pyramid-shaped maxillary sinus is the largest of the paranasal sinuses, located in the maxilla. It drains into the middle meatus of the nose through the semilunar hiatus. It is located to the side of the nasal cavity, and below the orbit.

A dental extraction is the removal of teeth from the dental alveolus (socket) in the alveolar bone. Extractions are performed for a wide variety of reasons, but most commonly to remove teeth which have become unrestorable through tooth decay, periodontal disease, or dental trauma, especially when they are associated with toothache. Sometimes impacted wisdom teeth cause recurrent infections of the gum (pericoronitis), and may be removed when other conservative treatments have failed. In orthodontics, if the teeth are crowded, healthy teeth may be extracted to create space so the rest of the teeth can be straightened.

The maxillary first molar is the human tooth located laterally from both the maxillary second premolars of the mouth but mesial from both maxillary second molars.
Dilaceration is a developmental disturbance in shape of teeth. It refers to an angulation, or a sharp bend or curve, in the root or crown of a formed tooth. This disturbance is more likely to affect the maxillary incisors and occurs in permanent dentition. Although this may seem more of an aesthetics issue, an impacted maxillary incisor will cause issues related to occlusion, phonetics, mastication, and psychology on young patients.

A buccal exostosis is an exostosis on the buccal surface of the alveolar ridge of the maxilla or mandible. More commonly seen in the maxilla than the mandible, buccal exostoses are considered to be site specific. Existing as asymptomatic bony nodules, buccal exostoses don’t usually present until adult life, and some consider buccal exostoses to be a variation of normal anatomy rather than disease. Bone is thought to become hyperplastic, consisting of mature cortical and trabecular bone with a smooth outer surface. They are less common when compared with mandibular tori.
Concrescence is an uncommon developmental condition of teeth where the cementum overlying the roots of at least two teeth fuse together without the involvement of dentin. Usually, two teeth are involved with the upper second and third molars being most commonly fused together. The prevalence ranges 0.04–0.8% in permanent teeth, with the incidence being highest in the posterior maxilla.
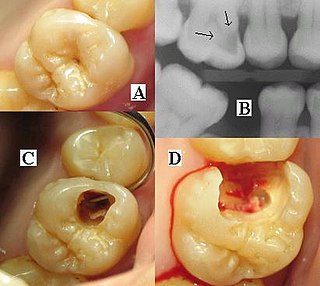
Dental radiographs, commonly known as X-rays, are radiographs used to diagnose hidden dental structures, malignant or benign masses, bone loss, and cavities.

Root canal treatment is a treatment sequence for the infected pulp of a tooth which is intended to result in the elimination of infection and the protection of the decontaminated tooth from future microbial invasion. Root canals, and their associated pulp chamber, are the physical hollows within a tooth that are naturally inhabited by nerve tissue, blood vessels and other cellular entities. Together, these items constitute the dental pulp.
Dental anesthesia is the application of anesthesia to dentistry. It includes local anesthetics, sedation, and general anesthesia.

An impacted tooth is one that fails to erupt into the dental arch within the expected developmental window. Because impacted teeth do not erupt, they are retained throughout the individual's lifetime unless extracted or exposed surgically. Teeth may become impacted because of adjacent teeth, dense overlying bone, excessive soft tissue or a genetic abnormality. Most often, the cause of impaction is inadequate arch length and space in which to erupt. That is the total length of the alveolar arch is smaller than the tooth arch. The wisdom teeth are frequently impacted because they are the last teeth to erupt in the oral cavity. Mandibular third molars are more commonly impacted than their maxillary counterparts.
Inferior alveolar nerve block is a nerve block technique which induces anesthesia (numbness) in the areas of the mouth and face innervated by one of the inferior alveolar nerves which are paired on the left and right side. These areas are the skin and mucous membranes of the lower lip, the skin of the chin, the lower teeth and the labial gingiva of the anterior teeth, all unilaterally to the midline of the side on which the block is administered. However, depending on technique, the long buccal nerve may not be anesthetized by an IANB and therefore an area of buccal gingiva adjacent to the lower posterior teeth will retain normal sensation unless that nerve is anesthetized separately, via a (long) buccal nerve block. The inferior alveolar nerve is a branch of the mandibular nerve, the third division of the trigeminal nerve. This procedure attempts to anaesthetise the inferior alveolar nerve prior to it entering the mandibular foramen on the medial surface of the mandibular ramus.

A panoramic radiograph is a panoramic scanning dental X-ray of the upper and lower jaw. It shows a two-dimensional view of a half-circle from ear to ear. Panoramic radiography is a form of focal plane tomography; thus, images of multiple planes are taken to make up the composite panoramic image, where the maxilla and mandible are in the focal trough and the structures that are superficial and deep to the trough are blurred.
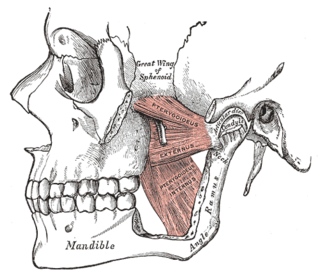
The pterygomandibular space is a fascial space of the head and neck. It is a potential space in the head and is paired on each side. It is located between the lateral pterygoid muscle and the medial surface of the ramus of the mandible. The pterygomandibular space is one of the four compartments of the masticator space.

Impacted wisdom teeth is a condition where the third molars are prevented from erupting into the mouth. This can be caused by a physical barrier, such as other teeth, or when the tooth is angled away from a vertical position. Completely unerupted wisdom teeth usually result in no symptoms, although they can sometimes develop cysts or neoplasms. Partially erupted wisdom teeth or wisdom teeth that are not erupted but are exposed to oral bacteria through deep periodontal pocket, can develop cavities or pericoronitis. Removal of impacted wisdom teeth is advised for the future prevention of or in the current presence of certain pathologies, such as caries, periodontal disease or cysts. Prophylactic (preventative) extraction of wisdom teeth is preferred to be done at a younger age to take advantage of incomplete root development, which is associated with an easier surgical procedure and less probability of complications.

Oroantral fistula (OAF) is an epithelialised oroantral communication (OAC). OAC refers to an abnormal connection between the oral cavity and antrum. The creation of an OAC is most commonly due to the extraction of a maxillary (upper) tooth closely related to the antral floor. A small OAC may heal spontaneously but a larger OAC would require surgical closure to prevent the development of persistent OAF and chronic sinusitis.
Alveoloplasty is a surgical pre-prosthetic procedure performed to facilitate removal of teeth, and smoothen or reshape the jawbone for prosthetic and cosmetic purposes. In this procedure, the bony edges of the alveolar ridge and its surrounding structures is made smooth, redesigned or recontoured so that a well-fitting, comfortable, and esthetic prosthesis may be fabricated or implants may be surgically inserted. This pre-prosthetic surgery which may include bone grafting prepares the mouth to receive a prosthesis or implants by improving the condition and quality of the supporting structures so they can provide support, better retention and stability to the prosthesis.
In the dental specialty of endodontics, periradicular surgery is surgery to the external root surface. Examples of periradicular surgery include apicoectomy, root resection, repair of root perforation or resorption defects, removal of broken fragments of the tooth or a filling material, and exploratory surgery to look for root fractures.
