An eating disorder is a mental disorder defined by abnormal eating behaviors that negatively affect a person's physical or mental health. Types of eating disorders include binge eating disorder, where the patient eats a large amount in a short period of time; anorexia nervosa, where the person has an intense fear of gaining weight and restricts food or overexercises to manage this fear; bulimia nervosa, where individuals eat a large quantity (binging) then try to rid themselves of the food (purging); pica, where the patient eats non-food items; rumination syndrome, where the patient regurgitates undigested or minimally digested food; avoidant/restrictive food intake disorder (ARFID), where people have a reduced or selective food intake due to some psychological reasons; and a group of other specified feeding or eating disorders. Anxiety disorders, depression and substance abuse are common among people with eating disorders. These disorders do not include obesity. People often experience comorbidity between an eating disorder and OCD. It is estimated 20–60% of patients with an ED have a history of OCD.

Bulimia nervosa, also known as simply bulimia, is an eating disorder characterized by binge eating followed by purging or fasting, and excessive concern with body shape and weight. This activity aims to expel the body of calories eaten from the binging phase of the process. Binge eating refers to eating a large amount of food in a short amount of time. Purging refers to the attempts to get rid of the food consumed. This may be done by vomiting or taking laxatives.
Binge eating disorder (BED) is an eating disorder characterized by frequent and recurrent binge eating episodes with associated negative psychological and social problems, but without the compensatory behaviors common to bulimia nervosa, OSFED, or the binge-purge subtype of anorexia nervosa.
Binge eating is a pattern of disordered eating which consists of episodes of uncontrollable eating. It is a common symptom of eating disorders such as binge eating disorder and bulimia nervosa. During such binges, a person rapidly consumes an excessive quantity of food. A diagnosis of binge eating is associated with feelings of loss of control. Binge eating disorder is also linked with being overweight and obesity.
Overeating occurs when an individual consumes more calories in relation to the energy that is expended via physical activity or expelled via excretion, leading to weight gain and often obesity. Overeating is the defining characteristic of binge eating disorder.
Muscle dysmorphia is a subtype of the obsessive mental disorder body dysmorphic disorder, but is often also grouped with eating disorders. In muscle dysmorphia, which is sometimes called "bigorexia", "megarexia", or "reverse anorexia", the delusional or exaggerated belief is that one's own body is too small, too skinny, insufficiently muscular, or insufficiently lean, although in most cases, the individual's build is normal or even exceptionally large and muscular already.
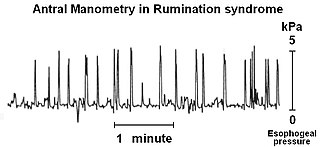
Rumination syndrome, or merycism, is a chronic motility disorder characterized by effortless regurgitation of most meals following consumption, due to the involuntary contraction of the muscles around the abdomen. There is no retching, nausea, heartburn, odour, or abdominal pain associated with the regurgitation as there is with typical vomiting, and the regurgitated food is undigested. The disorder has been historically documented as affecting only infants, young children, and people with cognitive disabilities . It is increasingly being diagnosed in a greater number of otherwise healthy adolescents and adults, though there is a lack of awareness of the condition by doctors, patients, and the general public.
The Eating Attitudes Test, created by David Garner, is a widely used 26-item, standardized self-reported questionnaire of symptoms and concerns characteristic of eating disorders. The EAT is useful in assessing "eating disorder risk" in high school, college and other special risk samples such as athletes. EAT has been extremely effective in screening for anorexia nervosa in many populations.
Ellen West (1888–1921) was a patient of Dr. Ludwig Binswanger who had anorexia nervosa. She became a famous example of Daseinsanalysis who died by suicide at age 33 by poisoning herself.
Diabulimia, also known as ED-DMT1 in the US or T1ED in the UK, is an eating disorder in which people with type 1 diabetes deliberately give themselves less insulin than they need or stop taking it altogether for the purpose of weight loss. Diabulimia is not recognized as a formal psychiatric diagnosis in the DSM-5. Because of this, some in the medical or psychiatric communities use the phrases "disturbed eating behavior" or "disordered eating behavior" and disordered eating (DE) are quite common in medical and psychiatric literature addressing patients who have type 1 diabetes and manipulate insulin doses to control weight along with exhibiting bulimic behavior.
Purging disorder is an eating disorder characterized by the DSM-5 as self-induced vomiting, or misuse of laxatives, diuretics, or enemas to forcefully evacuate matter from the body. Purging disorder differs from bulimia nervosa (BN) because individuals do not consume a large amount of food before they purge. In current diagnostic systems, purging disorder is a form of other specified feeding or eating disorder. Research indicates that purging disorder, while not rare, is not as commonly found as anorexia nervosa or bulimia nervosa. This syndrome is associated with clinically significant levels of distress, and that it appears to be distinct from bulimia nervosa on measures of hunger and ability to control food intake. Some of the signs of purging disorder are frequent trips to the bathroom directly after a meal, frequent use of laxatives, and obsession over one's appearance and weight. Other signs include swollen cheeks, popped blood vessels in the eyes, and clear teeth which are all signs of excessive vomiting.
Maudsley family therapy also known as family-based treatment or Maudsley approach, is a family therapy for the treatment of anorexia nervosa devised by Christopher Dare and colleagues at the Maudsley Hospital in London. A comparison of family to individual therapy was conducted with eighty anorexia patients. The study showed family therapy to be the more effective approach in patients under 18 and within 3 years of the onset of their illness. Subsequent research confirmed the efficacy of family-based treatment for teens with anorexia nervosa. Family-based treatment has been adapted for bulimia nervosa and showed promising results in a randomized controlled trial comparing it to supportive individual therapy.

Anorexia nervosa (AN), often referred to simply as anorexia, is an eating disorder characterized by food restriction, body image disturbance, fear of gaining weight, and an overpowering desire to be thin.
The differential diagnoses of anorexia nervosa (AN) includes various types of medical and psychological conditions, which may be misdiagnosed as AN. In some cases, these conditions may be comorbid with AN because the misdiagnosis of AN is not uncommon. For example, a case of achalasia was misdiagnosed as AN and the patient spent two months confined to a psychiatric hospital. A reason for the differential diagnoses that surround AN arise mainly because, like other disorders, it is primarily, albeit defensively and adaptive for, the individual concerned. Anorexia Nervosa is a psychological disorder characterized by extremely reduced intake of food. People with anorexia nervosa tend to have a low self-image and an inaccurate perception of their body.

Many memory impairments exist as a result from or cause of eating disorders. Eating disorders (EDs) are characterized by abnormal and disturbed eating patterns that affect the lives of the individuals who worry about their weight to the extreme. These abnormal eating patterns involve either inadequate or excessive food intake, affecting the individual's physical and mental health.
Cognitive behavioral therapy (CBT) is derived from both the cognitive and behavioral schools of psychology and focuses on the alteration of thoughts and actions with the goal of treating various disorders. The cognitive behavioral treatment of eating disorders emphasizes on the minimization of negative thoughts about body image and the act of eating, and attempts to alter negative and harmful behaviors that are involved in and perpetuate eating disorders. It also encourages the ability to tolerate negative thoughts and feelings as well as the ability to think about food and body perception in a multi-dimensional way. The emphasis is not only placed on altering cognition, but also on tangible practices like making goals and being rewarded for meeting those goals. CBT is a "time-limited and focused approach" which means that it is important for the patients of this type of therapy to have particular issues that they want to address when they begin treatment. CBT has also proven to be one of the most effective treatments for eating disorders.
Cognitive emotional behavioral therapy (CEBT) is an extended version of cognitive behavioral therapy (CBT) aimed at helping individuals to evaluate the basis of their emotional distress and thus reduce the need for associated dysfunctional coping behaviors. This psychotherapeutic intervention draws on a range of models and techniques including dialectical behavior therapy (DBT), mindfulness meditation, acceptance and commitment therapy (ACT), and experiential exercises.
Body image disturbance (BID) is a common symptom in patients with eating disorders and is characterized by an altered perception of one's own body.
Atypical anorexia nervosa is an eating disorder in which individuals meet all the qualifications for anorexia nervosa, including a body image disturbance and a history of restrictive eating and weight loss, except that they are not currently underweight. Atypical anorexia qualifies as a mental health disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), under the category Other Specified Feeding and Eating Disorders (OSFED). The characteristics of people with atypical anorexia generally do not differ significantly from anorexia nervosa patients except for their current weight.
Body checking is a compulsive behaviour related but not exclusive to various forms of body dysmorphic disorders. It involves frequently collecting various information about one’s own body in terms of size, shape, appearance or weight. Frequent expressions of this form of behaviour entails for example mirror checking, trying to feel one’s own bones, pinching the abdomen, frequent body weight measurement and comparing your own body to that of others. Studies have shown that an increased rate of body checking correlates with an overall increased dissatisfaction with the own body.