
Agnosia is the inability to process sensory information. Often there is a loss of ability to recognize objects, persons, sounds, shapes, or smells while the specific sense is not defective nor is there any significant memory loss. It is usually associated with brain injury or neurological illness, particularly after damage to the occipitotemporal border, which is part of the ventral stream. Agnosia only affects a single modality, such as vision or hearing. More recently, a top-down interruption is considered to cause the disturbance of handling perceptual information.

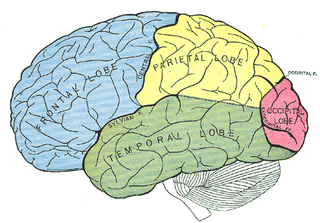
The parietal lobe is one of the four major lobes of the cerebral cortex in the brain of mammals. The parietal lobe is positioned above the temporal lobe and behind the frontal lobe and central sulcus.

Prosopagnosia, also called face blindness, is a cognitive disorder of face perception in which the ability to recognize familiar faces, including one's own face (self-recognition), is impaired, while other aspects of visual processing and intellectual functioning remain intact. The term originally referred to a condition following acute brain damage, but a congenital or developmental form of the disorder also exists, with a prevalence of 2.5%. The brain area usually associated with prosopagnosia is the fusiform gyrus, which activates specifically in response to faces. The functionality of the fusiform gyrus allows most people to recognize faces in more detail than they do similarly complex inanimate objects. For those with prosopagnosia, the method for recognizing faces depends on the less sensitive object-recognition system. The right hemisphere fusiform gyrus is more often involved in familiar face recognition than the left. It remains unclear whether the fusiform gyrus is specific for the recognition of human faces or if it is also involved in highly trained visual stimuli.
Split-brain or callosal syndrome is a type of disconnection syndrome when the corpus callosum connecting the two hemispheres of the brain is severed to some degree. It is an association of symptoms produced by disruption of, or interference with, the connection between the hemispheres of the brain. The surgical operation to produce this condition involves transection of the corpus callosum, and is usually a last resort to treat refractory epilepsy. Initially, partial callosotomies are performed; if this operation does not succeed, a complete callosotomy is performed to mitigate the risk of accidental physical injury by reducing the severity and violence of epileptic seizures. Before using callosotomies, epilepsy is instead treated through pharmaceutical means. After surgery, neuropsychological assessments are often performed.
Astereognosis is the inability to identify an object by active touch of the hands without other sensory input, such as visual or sensory information. An individual with astereognosis is unable to identify objects by handling them, despite intact elementary tactile, proprioceptive, and thermal sensation. With the absence of vision, an individual with astereognosis is unable to identify what is placed in their hand based on cues such as texture, size, spatial properties, and temperature. As opposed to agnosia, when the object is observed visually, one should be able to successfully identify the object.

Hemispatial neglect is a neuropsychological condition in which, after damage to one hemisphere of the brain, a deficit in attention and awareness towards the side of space opposite brain damage is observed. It is defined by the inability of a person to process and perceive stimuli towards the contralesional side of the body or environment. Hemispatial neglect is very commonly contralateral to the damaged hemisphere, but instances of ipsilesional neglect have been reported.
Bálint's syndrome is an uncommon and incompletely understood triad of severe neuropsychological impairments: inability to perceive the visual field as a whole (simultanagnosia), difficulty in fixating the eyes, and inability to move the hand to a specific object by using vision. It was named in 1909 for the Austro-Hungarian neurologist and psychiatrist Rezső Bálint who first identified it.

Visual memory describes the relationship between perceptual processing and the encoding, storage and retrieval of the resulting neural representations. Visual memory occurs over a broad time range spanning from eye movements to years in order to visually navigate to a previously visited location. Visual memory is a form of memory which preserves some characteristics of our senses pertaining to visual experience. We are able to place in memory visual information which resembles objects, places, animals or people in a mental image. The experience of visual memory is also referred to as the mind's eye through which we can retrieve from our memory a mental image of original objects, places, animals or people. Visual memory is one of several cognitive systems, which are all interconnected parts that combine to form the human memory. Types of palinopsia, the persistence or recurrence of a visual image after the stimulus has been removed, is a dysfunction of visual memory.

Associative visual agnosia is a form of visual agnosia. It is an impairment in recognition or assigning meaning to a stimulus that is accurately perceived and not associated with a generalized deficit in intelligence, memory, language or attention. The disorder appears to be very uncommon in a "pure" or uncomplicated form and is usually accompanied by other complex neuropsychological problems due to the nature of the etiology. Affected individuals can accurately distinguish the object, as demonstrated by the ability to draw a picture of it or categorize accurately, yet they are unable to identify the object, its features or its functions.
Visual agnosia is an impairment in recognition of visually presented objects. It is not due to a deficit in vision, language, memory, or intellect. While cortical blindness results from lesions to primary visual cortex, visual agnosia is often due to damage to more anterior cortex such as the posterior occipital and/or temporal lobe(s) in the brain.[2] There are two types of visual agnosia: apperceptive agnosia and associative agnosia.
Mirrored-self misidentification is the delusional belief that one's reflection in the mirror is another person – typically a younger or second version of one's self, a stranger, or a relative. This delusion occurs most frequently in patients with dementia and an affected patient maintains the ability to recognize others' reflections in the mirror. It is caused by right hemisphere cranial dysfunction that results from traumatic brain injury, stroke, or general neurological illness. It is an example of a monothematic delusion, a condition in which all abnormal beliefs have one common theme, as opposed to a polythematic delusion, in which a variety of unrelated delusional beliefs exist. This delusion is also classified as one of the delusional misidentification syndromes (DMS). A patient with a DMS condition consistently misidentifies places, objects, persons, or events. DMS patients are not aware of their psychological condition, are resistant to correction and their conditions are associated with brain disease – particularly right hemisphere brain damage and dysfunction.
Autotopagnosia from the Greek a and gnosis, meaning "without knowledge", topos meaning "place", and auto meaning "oneself", autotopagnosia virtually translates to the "lack of knowledge about one's own space," and is clinically described as such.

Integrative agnosia is a sub-disease of agnosia, meaning the lack of integrating perceptual wholes within knowledge. Integrative agnosia can be assessed by several experimental tests such as the Efron shape test, which determines the specificity of the disease being Integrative. This disease is often caused by brain trauma, producing medial ventral lesions to the extrastriate cortex. Affecting this region of the brain produces learning impairments: the inability to integrate parts such as spatial distances or producing visual images from short or long-term memory.
Apperceptive agnosia is a failure in recognition that is due to a failure of perception. In contrast, associative agnosia is a type of agnosia where perception occurs but recognition still does not occur. When referring to apperceptive agnosia, visual and object agnosia are most commonly discussed; this occurs because apperceptive agnosia is most likely to present visual impairments. However, in addition to visual apperceptive agnosia there are also cases of apperceptive agnosia in other sensory areas.
Visual object recognition refers to the ability to identify the objects in view based on visual input. One important signature of visual object recognition is "object invariance", or the ability to identify objects across changes in the detailed context in which objects are viewed, including changes in illumination, object pose, and background context.
Amorphosynthesis, also called a hemi-sensory deficit, is a neuropsychological condition in which a patient experiences unilateral inattention to sensory input. This phenomenon is frequently associated with damage to the right cerebral hemisphere resulting in severe sensory deficits that are observed on the contralesional (left) side of the body. A right-sided deficit is less commonly observed and the effects are reported to be temporary and minor. Evidence suggests that the right cerebral hemisphere has a dominant role in attention and awareness to somatic sensations through ipsilateral and contralateral stimulation. In contrast, the left cerebral hemisphere is activated only by contralateral stimuli. Thus, the left and right cerebral hemispheres exhibit redundant processing to the right-side of the body and a lesion to the left cerebral hemisphere can be compensated by the ipsiversive processes of the right cerebral hemisphere. For this reason, right-sided amorphosynthesis is less often observed and is generally associated with bilateral lesions.
Constructional apraxia is characterized by an inability or difficulty to build, assemble, or draw objects. Apraxia is a neurological disorder in which people are unable to perform tasks or movements even though they understand the task, are willing to complete it, and have the physical ability to perform the movements. Constructional apraxia may be caused by lesions in the parietal lobe following stroke or it may serve as an indicator for Alzheimer's disease.
Topographical disorientation is the inability to orient oneself in one's surroundings, sometimes as a result of focal brain damage. This disability may result from the inability to make use of selective spatial information or to orient by means of specific cognitive strategies such as the ability to form a mental representation of the environment, also known as a cognitive map. It may be part of a syndrome known as visuospatial dysgnosia.
Haptic memory is the form of sensory memory specific to touch stimuli. Haptic memory is used regularly when assessing the necessary forces for gripping and interacting with familiar objects. It may also influence one's interactions with novel objects of an apparently similar size and density. Similar to visual iconic memory, traces of haptically acquired information are short lived and prone to decay after approximately two seconds. Haptic memory is best for stimuli applied to areas of the skin that are more sensitive to touch. Haptics involves at least two subsystems; cutaneous, or everything skin related, and kinesthetic, or joint angle and the relative location of body. Haptics generally involves active, manual examination and is quite capable of processing physical traits of objects and surfaces.
Form perception is the recognition of visual elements of objects, specifically those to do with shapes, patterns and previously identified important characteristics. An object is perceived by the retina as a two-dimensional image,[1] but the image can vary for the same object in terms of the context with which it is viewed, the apparent size of the object, the angle from which it is viewed, how illuminated it is, as well as where it resides in the field of vision.[2] Despite the fact that each instance of observing an object leads to a unique retinal response pattern, the visual processing in the brain is capable of recognizing these experiences as analogous, allowing invariant object recognition. recognition|object recognition]]. Visual processing occurs in a hierarchy with the lowest levels recognizing lines and contours, and slightly higher levels performing tasks such as completing boundaries and recognizing contour combinations. The highest levels integrate the perceived information to recognize an entire object. Essentially object recognition is the ability to assign labels to objects in order to categorize and identify them, thus distinguishing one object from another. During visual processing information is not created, but rather reformatted in a way that draws out the most detailed information of the stimulus.