Ataxia is a neurological sign consisting of lack of voluntary coordination of muscle movements that can include gait abnormality, speech changes, and abnormalities in eye movements. Ataxia is a clinical manifestation indicating dysfunction of the parts of the nervous system that coordinate movement, such as the cerebellum. Ataxia can be limited to one side of the body, which is referred to as hemiataxia. Several possible causes exist for these patterns of neurological dysfunction. Dystaxia is a mild degree of ataxia. Friedreich's ataxia has gait abnormality as the most commonly presented symptom. The word is from Greek α- [a negative prefix] + -τάξις [order] = "lack of order".
In neuroscience, an F wave is one of several motor responses which may follow the direct motor response (M) evoked by electrical stimulation of peripheral motor or mixed nerves. F-waves are the second of two late voltage changes observed after stimulation is applied to the skin surface above the distal region of a nerve, in addition to the H-reflex which is a muscle reaction in response to electrical stimulation of innervating sensory fibers. Traversal of F-waves along the entire length of peripheral nerves between the spinal cord and muscle, allows for assessment of motor nerve conduction between distal stimulation sites in the arm and leg, and related motoneurons (MN's) in the cervical and lumbosacral cord. F-waves are able to assess both afferent and efferent loops of the alpha motor neuron in its entirety. As such, various properties of F-wave motor nerve conduction are analyzed in nerve conduction studies (NCS), and often used to assess polyneuropathies, resulting from states of neuronal demyelination and loss of peripheral axonal integrity.

The Valsalva maneuver is performed by a forceful attempt of exhalation against a closed airway, usually done by closing one's mouth and pinching one's nose shut while expelling air out as if blowing up a balloon. Variations of the maneuver can be used either in medical examination as a test of cardiac function and autonomic nervous control of the heart, or to clear the ears and sinuses when ambient pressure changes, as in scuba diving, hyperbaric oxygen therapy, or air travel.
The ankle jerk reflex, also known as the Achilles reflex, occurs when the Achilles tendon is tapped while the foot is dorsiflexed. It is a type of stretch reflex that tests the function of the gastrocnemius muscle and the nerve that supplies it. A positive result would be the jerking of the foot towards its plantar surface. Being a deep tendon reflex, it is monosynaptic. It is also a stretch reflex. These are monosynaptic spinal segmental reflexes. When they are intact, integrity of the following is confirmed: cutaneous innervation, motor supply, and cortical input to the corresponding spinal segment.
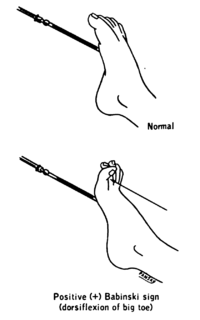
The plantar reflex is a reflex elicited when the sole of the foot is stimulated with a blunt instrument. The reflex can take one of two forms. In healthy adults, the plantar reflex causes a downward response of the hallux (flexion). An upward response (extension) of the hallux is known as the Babinski response or Babinski sign, named after the neurologist Joseph Babinski. The presence of the Babinski sign can identify disease of the spinal cord and brain in adults, and also exists as a primitive reflex in infants.

Functional electrical stimulation (FES) is a technique that uses low-energy electrical pulses to artificially generate body movements in individuals who have been paralyzed due to injury to the central nervous system. More specifically, FES can be used to generate muscle contraction in otherwise paralyzed limbs to produce functions such as grasping, walking, bladder voiding and standing. This technology was originally used to develop neuroprostheses that were implemented to permanently substitute impaired functions in individuals with spinal cord injury (SCI), head injury, stroke and other neurological disorders. In other words, a person would use the device each time he or she wanted to generate a desired function. FES is sometimes also referred to as neuromuscular electrical stimulation (NMES).

The patellar reflex, also called the knee reflex or knee-jerk, is a stretch reflex which tests the L2, L3, and L4 segments of the spinal cord.

The acoustic reflex is an involuntary muscle contraction that occurs in the middle ear in response to loud sound stimuli or when the person starts to vocalize.

The Moro reflex is an infantile reflex that develops between 28 and 32 weeks of gestation and disappears at 3–6 months of age. It is a response to a sudden loss of support and involves three distinct components:
- spreading out the arms (abduction)
- pulling the arms in (adduction)
- crying (usually)

Blepharospasm is any abnormal contraction of the orbicularis oculi muscle. The condition should be distinguished from the more common, and milder, involuntary quivering of an eyelid, known as myokymia, or fasciculation. In most cases, blepharospasm symptoms last for a few days and then disappear without treatment, but in some cases the twitching is chronic and persistent, causing life-long challenges. In these cases, the symptoms are often severe enough to result in functional blindness. The person's eyelids feel like they are clamping shut and will not open without great effort. People have normal eyes, but for periods of time are effectively blind due to their inability to open their eyelids. In contrast, the reflex blepharospasm is due to any pain in and around the eye.

The scratch reflex is a response to activation of sensory neurons whose peripheral terminals are located on the surface of the body. Some sensory neurons can be activated by stimulation with an external object such as a parasite on the body surface. Alternatively, some sensory neurons can respond to a chemical stimulus that produces an itch sensation. During a scratch reflex, a nearby limb reaches toward and rubs against the site on the body surface that has been stimulated. The scratch reflex has been extensively studied to understand the functioning of neural networks in vertebrates. Despite decades of research, key aspects of the scratch reflex are still unknown, such as the neural mechanisms by which the reflex is terminated.
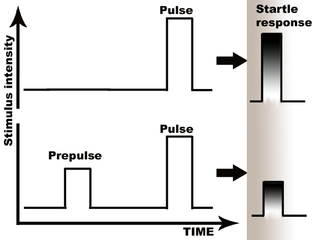
Prepulse inhibition (PPI) is a neurological phenomenon in which a weaker prestimulus (prepulse) inhibits the reaction of an organism to a subsequent strong reflex-eliciting stimulus (pulse), often using the startle reflex. The stimuli are usually acoustic, but tactile stimuli and light stimuli are also used. When prepulse inhibition is high, the corresponding one-time startle response is reduced.
Pupilometer, also spelled pupillometer, is a name for two different devices—one used to measure the pupillary light reflex, and the other used in ophthalmology, which measures the distance between pupils through visual stimuli.

The stretch reflex, or more accurately "muscle stretch reflex", is a muscle contraction in response to stretching within the muscle. The reflex functions to maintain the muscle at a constant length. The term deep tendon reflex is often wrongfully used by many health workers and students to refer to this reflex. "Tendons have little to do with the response, other than being responsible for mechanically transmitting the sudden stretch from the reflex hammer to the muscle spindle. In addition, some muscles with stretch reflexes have no tendons ".

A reflex hammer is a medical instrument used by practitioners to test deep tendon reflexes. Testing for reflexes is an important part of the neurological physical examination in order to detect abnormalities in the central or peripheral nervous system.
Central facial palsy is a symptom or finding characterized by paralysis or paresis of the lower half of one side of the face. It usually results from damage to upper motor neurons of the facial nerve.
Hoffmann's reflex is a neurological examination finding elicited by a reflex test which can help verify the presence or absence of issues arising from the corticospinal tract. It is named after neurologist Johann Hoffmann. Usually considered a pathological reflex in a clinical setting, the Hoffmann's reflex has also been used as a measure of spinal reflex processing (adaptation) in response to exercise training.

Jendrassik Ernő was a Hungarian physician best known for his research on reflexes, in particular, the Jendrassik maneuver.
Sunil Pradhan is an Indian neurologist, medical researcher and writer, known for the invention of two electrophysiological techniques. He has also described five medical signs, of which one related to Duchenne muscular dystrophy is known as Pradhan Sign, and the others associated with facioscapulohumeral muscular dystrophy (FSHD) and similar neuro diseases. The Government of India awarded him the Padma Shri, the fourth highest civilian award, in 2014 for his contributions to the field of neuroscience.

An upper limb neurological examination is part of the neurological examination, and is used to assess the motor and sensory neurons which supply the upper limbs. This assessment helps to detect any impairment of the nervous system, being used both as a screening and an investigative tool. The examination findings when combined with a detailed history of a patient, can help a doctor reach a specific or differential diagnosis. This would enable the doctor to commence treatment if a specific diagnosis has been made, or order further investigations if there are differential diagnoses.

{kind=link}