Related Research Articles
Orthodontics is a dentistry specialty that addresses the diagnosis, prevention, management, and correction of mal-positioned teeth and jaws, as well as misaligned bite patterns. It may also address the modification of facial growth, known as dentofacial orthopedics.

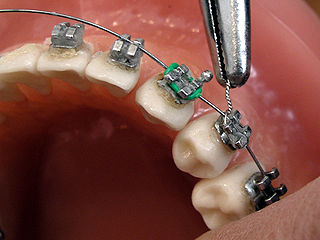
Dental braces are devices used in orthodontics that align and straighten teeth and help position them with regard to a person's bite, while also aiming to improve dental health. They are often used to correct underbites, as well as malocclusions, overbites, open bites, gaps, deep bites, cross bites, crooked teeth, and various other flaws of the teeth and jaw. Braces can be either cosmetic or structural. Dental braces are often used in conjunction with other orthodontic appliances to help widen the palate or jaws and to otherwise assist in shaping the teeth and jaws.

Clear aligners are orthodontic devices that are a transparent, plastic form of dental braces used to adjust teeth.
Hypodontia is defined as the developmental absence of one or more teeth excluding the third molars. It is one of the most common dental anomalies, and can have a negative impact on function, and also appearance. It rarely occurs in primary teeth and the most commonly affected are the adult second premolars and the upper lateral incisors. It usually occurs as part of a syndrome that involves other abnormalities and requires multidisciplinary treatment.

In orthodontics, a malocclusion is a misalignment or incorrect relation between the teeth of the upper and lower dental arches when they approach each other as the jaws close. The English-language term dates from 1864; Edward Angle (1855–1930), the "father of modern orthodontics", popularised it. The word derives from mal- 'incorrect' and occlusion 'the manner in which opposing teeth meet'.

A palatal expander is a device in the field of orthodontics which is used to widen the upper jaw (maxilla) so that the bottom and upper teeth will fit together better. This is a common orthodontic procedure. The use of an expander is most common in children and adolescents 8–18 years of age. It can also be used in adults, although expansion is more uncomfortable and takes longer in adults. A patient who would rather not wait several months for the end result achieved by a palatal expander may be able to opt for a surgical separation of the maxilla. Use of a palatal expander is most often followed by braces to then straighten the teeth.
Orthodontic technology is a specialty of dental technology that is concerned with the design and fabrication of dental appliances for the treatment of malocclusions, which may be a result of tooth irregularity, disproportionate jaw relationships, or both.

Tooth eruption is a process in tooth development in which the teeth enter the mouth and become visible. It is currently believed that the periodontal ligament plays an important role in tooth eruption. The first human teeth to appear, the deciduous (primary) teeth, erupt into the mouth from around 6 months until 2 years of age, in a process known as "teething". These teeth are the only ones in the mouth until a person is about 6 years old creating the primary dentition stage. At that time, the first permanent tooth erupts and begins a time in which there is a combination of primary and permanent teeth, known as the mixed dentition stage, which lasts until the last primary tooth is lost. Then, the remaining permanent teeth erupt into the mouth during the permanent dentition stage.

In dentistry, overjet is the extent of horizontal (anterior-posterior) overlap of the maxillary central incisors over the mandibular central incisors. In class II malocclusion the overjet is increased as the maxillary central incisors are protruded.

In dentistry, crossbite is a form of malocclusion where a tooth has a more buccal or lingual position than its corresponding antagonist tooth in the upper or lower dental arch. In other words, crossbite is a lateral misalignment of the dental arches.
Serial extraction is the planned extraction of certain deciduous teeth and specific permanent teeth in an orderly sequence and predetermined pattern to guide the erupting permanent teeth into a more favorable position.
Lingual braces are one of the many types of the fixed orthodontic treatment appliances available to patients needing orthodontics. They involve attaching the orthodontic brackets on the inner sides of the teeth. The main advantage of lingual braces is their near invisibility compared to the standard braces, which are attached on the buccal (cheek) sides of the tooth. Lingual braces were invented by Craven Kurz in 1976.
Tooth ankylosis refers to a fusion between a tooth and underlying bony support tissues. In some species, this is a normal process that occurs during the formation or maintenance of the dentition. By contrast, in humans tooth ankylosis is pathological, whereby a fusion between alveolar bone and the cementum of a tooth occurs.
Hayes Nance was an American orthodontist known for his contributions to topics related to mixed dentition. Nance is known for developing serial extraction in United States, as well as pioneering the development of the Nance Appliance.
A lip bumper is a dental appliance used in orthodontics, for various purposes to correct a dentition by preventing the pressure from the soft tissue. Lip bumpers are usually used in orthodontic treatment where the patient has a crowded maxillary or mandibular teeth in an arch.
Activator Appliance is an Orthodontics appliance that was developed by Viggo Andresen in 1908. This was one of the first functional appliances that was developed to correct functional jaw in the early 1900s. Activator appliance became the universal appliance that was used widely throughout Europe in the earlier part of the 20th century.
Open bite is a type of orthodontic malocclusion which has been estimated to occur in 0.6% of the people in the United States. This type of malocclusion has no vertical overlap or contact between the anterior incisors. The term "open bite" was coined by Carevelli in 1842 as a distinct classification of malocclusion. Different authors have described the open bite in a variety of ways. Some authors have suggested that open bite often arises when overbite is less than the usual amount. Additionally, others have contended that open bite is identified by end-on incisal relationships. Lastly, some researchers have stated that a lack of incisal contact must be present to diagnose an open bite.
An ectopic maxillary canine is a canine which is following abnormal path of eruption in the maxilla. An impacted tooth is one which is blocked from erupting by a physical barrier in the path of eruption. Ectopic eruption may lead to impaction. Previously, it was assumed that 85% of ectopic canines are displaced palatally, however a recent study suggests the true occurrence is closer to 50%. While maxillary canines can also be displaced buccally, it is thought this arises as a result of a lack of space. Most of these cases resolve themselves with the permanent canine erupting without intervention.
Orthodontic indices are one of the tools that are available for orthodontists to grade and assess malocclusion. Orthodontic indices can be useful for an epidemiologist to analyse prevalence and severity of malocclusion in any population.
The Herbst appliance is an orthodontic appliance used by orthodontists to correct class 2 retrognathic mandible in a growing patient, meaning that the lower jaw is too far back. This is also called bitejumping. Herbst appliance parts include stainless steel surgical frameworks that are secured onto the teeth by bands or acrylic bites. These are connected by sets of telescoping mechanisms that apply gentle upward and backward force on the upper jaw, and forward force on the lower jaw. The original bite-jumping appliance was designed by Dr. Emil Herbst and reintroduced by Dr. Hans Pancherz using maxillary and mandibular first molars and first bicuspids. The bands were connected with heavy wire soldered to each band and carried a tube and piston assembly that allowed mandibular movement but permanently postured the mandible forward. The appliance not only corrected a dental Class II to a dental Class I but also offered a marked improvement of the classic Class II facial profile.
References
- ↑ American Journal of Orthodontics and DentoFacial Orthopedics "Preventive Treatment of Ectopically Erupting Maxillary Permanent Canines by Extraction of Deciduous Canines and First Molars: A Randomized Clinical Trial" March 2011. http://www.ajodo.org/article/S0889-5406(10)00764-X/abstract
- ↑ American Dental Association's Current Dental Terminology User's Manuel, 2012 Edition as CODE 8060 (Appendix 1), “Interceptive Orthodontic Treatment of the Transitional Dentition.” http://www.dhhs.nh.gov/ombp/medicaid/children/documents/dpm.pdf
- ↑ The guidance of Eruption Without Extraction: http://ejo.oxfordjournals.org/content/29/suppl_1/i107.full
- ↑ Orthodontic braces
- ↑ Ngan, Peter W.; Kao, Elizabeth C.; Wei, Stephen H. (1 April 2003). "Guidance of eruption for general practitioners" (PDF). International Dental Journal. 53 (2): 100–113. doi:10.1111/j.1875-595x.2003.tb00667.x. PMID 12731698. Archived from the original (PDF) on 8 August 2014. Retrieved 27 February 2023.
- ↑ Dentofacial Changes after Orthodontic Intervention with Eruption Guidance Appliance in the Early Mixed Dentition: http://www.angle.org/doi/abs/10.2319/012607-37.1
- ↑ Treatment stability with the eruption guidance appliance. http://uningateresina.com.br/Dimon/Arquivos/Artigos/13279707934f2739e9e14b6.pdf