Smile surgery or smile reconstruction is a surgical procedure that restores the smile for people with facial nerve paralysis. Facial nerve paralysis is a relatively common condition with a yearly incidence of 0.25% leading to function loss of the mimic muscles.[1] The facial nerve gives off several branches in the face. If one or more facial nerve branches are paralysed, the corresponding mimetic muscles lose their ability to contract.[2] This may lead to several symptoms such as incomplete eye closure with or without exposure keratitis, oral incompetence, poor articulation, dental caries, drooling, and a low self-esteem.[3][4] This is because the different branches innervate the frontalis muscle, orbicularis oculi and oris muscles, lip elevators and depressors, and the platysma. The elevators of the upper lip and corner of the mouth are innervated by the zygomatic and buccal branches.[5] When these branches are paralysed, there is an inability to create a symmetric smile.[3]
Smile surgery is performed as a static or dynamic reconstruction. An example of static reconstruction is upper and lower lip shortening or thickening with commissure preservation.[6] Dynamic smile reconstruction procedures restore the facial nerve activity.
Historical background
The first known surgical repair of an injured facial nerve was performed by Drobnick in 1879, who connected the proximal spinal accessory nerve (innervates trapezius and sternocleidomastoid muscles) to the paralysed facial nerve. More symmetrical features were the result. In 1971 a new technique for facial nerve reconstruction was introduced, as Scaramella and Smith reported on the technique of cross facial nerve grafting (CFNG) for reconstruction of a coordinated smile in unilateral facial paralysis cases. Harii et al. for the first time used a free muscle transfer in combination with a nerve transfer in 1976. Eight years later, Terzis introduced the "babysitter" procedure, which consists of a combination of CFNGs and a simultaneous partial hypoglossal to facial nerve transfer. In 1989, Zuker et al. suggested the use of the masseteric nerve as possible donor nerve for innervation of the transplanted muscle in patients with Moebius syndrome.[2]
Indications
The main indications for dynamic smile reconstruction are unilateral or bilateral facial paralysis due to acquired and congenital causes.[2] Trauma, Bell's palsy and tumour extirpation are examples of secondary or acquired facial paralysis. Bell's palsy or idiopathic facial paralysis is a condition which leads to facial paralysis, however, without a known cause. It has an acute onset and is mostly self-limiting. But if spontaneous recurrence of (near) normal function does not take place, surgical reanimation may be indicated. Some head and neck tumours invade or compress the facial nerve leading to facial paresis or paralysis. Examples of such tumours are facial neuromas, cholesteatomas, hemangiomas, acoustic neuromas, parotid gland neoplasms or metastases. Sometimes, the facial nerve cannot be preserved during resection of these tumours.[citation needed]
Congenital facial paralysis occurs usually unilaterally and may be complete or incomplete. The most common congenital cause is the Moebius syndrome. Moebius syndrome is a congenital neurological disorder with bilateral paralysis of both the facial and abducens nerves. Therefore, lateral eye movement and facial animation are absent. In Moebius-like syndrome, only one side of the face is affected, but with additional nerve palsies of the affected facial and abducens nerve.[3]
Surgical techniques
1. Algorithm for dynamic smile reconstruction in acquired facial paralysis2. Algorithm for dynamic smile reconstruction in congenital facial paralysis
Selection of the type of nerve transfer is based on the individualised needs and condition of the patient. Individual factors can be patient age, type of paralysis (partial or complete, uni- or bilateral), denervation time of the mimetic muscles, availability of nerve grafts and medical condition of the patient.[2]
If facial paralysis is caused by trauma or tumour surgery, direct reinnervation of the facial muscles (ideally within 72 hours after facial nerve damage) can be achieved by neurorrhaphy, with or without an interposition nerve graft. (Algorithm 1)[7] Neurorrhaphy is a primary end-to-end reconnection of the facial nerve stumps.[8] However, tension-free reconnection is needed, otherwise scar formation can occur and axons will regenerate outside the facial nerve.[9] If a tension-free reconnection is not possible, interposition nerve grafts are an option.[8][9] Mostly the great auricular nerve or sural nerve is used as a graft between the two facial nerve stumps.[8]
Cross facial nerve graft
In more long standing acquired facial paralysis either a CFNG procedure or "babysitter" procedure are the indicated techniques, with or without a free muscle transfer.(Algorithm 1)[2] Secondary facial paralysis with a denervation time of less than 6 months can be treated with one or more cross facial nerve grafts (CFNGs).[2] During a cross facial nerve graft procedure one or more branches of the non-paralysed facial nerve are divided and connected to one or more sural nerve grafts which are tunnelled to the affected side of the face. Whether these nerve grafts are immediately attached to the paralysed facial nerve branches or after 9 to 12 months depends on the chosen procedure.[citation needed]
Babysitter procedure
If facial paralysis lasts between 6 months and 2 years, the "babysitter" procedure may be used.(Algorithm 1)[2] During this operation both CFNGs and part of an undamaged donor nerve on the affected side are used.[10] For example, the hypoglossal nerve[10] or masseteric nerve on the affected side can be used as donor nerves. This donor nerve is then attached to the distal end of the paralysed facial nerve.[5] A free muscle transplant is sometimes indicated after the "babysitter" procedure has been performed, depending on the continuity of the injured facial nerve. In other words, if there is contraction of the mimetic muscle during an electromyogram.[10] After a denervation time of approximately more than 2 years, atrophy of the mimetic muscles is permanent.[5] In these cases a free muscle transfer is always performed in combination with a CFNG.[2]
Motor donor nerve
The procedure of choice for congenital facial paralysis is either CFNG or motor donors, both with a free muscle transfer. (Algorithm 2) Incomplete bilateral Moebius syndrome has the same clinical features as the Moebius syndrome, however some motor function is still apparent on one side of the face.[3] This incomplete syndrome is reanimated with the use of the CFNG and free muscle transfer. The cross facial nerve graft comes from the side with some motor function of the facial nerve. However it first has to be investigated if the motor function of the nerve is strong enough to be separated.[2] A free muscle transfer is always used on the paralysed side, as the muscle is a congenital atrophic muscle. Complete bilateral Moebius syndrome is treated with motor donor nerves on both sides.[2][3] Optional motor donor nerves are: the masseteric nerve, accessory nerve or hypoglossal nerve. In rare cases when these nerves are also affected, cervical nerve branches can be used.[2] The use of a free muscle transfer is again indicated.[3] The nerve that initially innervated the free muscle transfer is then connected to the provided branches of the motor donor nerve. In Moebius-like syndrome the CFNG is performed, as the facial nerve on the affected side does not have a strong enough motor function. A free muscle transfer is also used, due to the atrophic muscle.[2][3]
Surgical procedures
Based on the preference of the surgeon, the gracilis muscle, latissimus dorsi muscle, or pectoralis minor muscle are used as free neurovascular grafts. The gracilis muscle is mostly used free neurovascular muscle, because it has a reliable anatomy and is relatively simple to harvest.[11] In addition, it can be trimmed for the correct size and volume[11] with preservation of superior contraction qualities compared to bipennate muscles, because the gracilis is a parallel-fibered or strap muscle.[12] Another advantage is the possibility for simultaneous dissection by a second team while the first team is preparing the face for the free muscle transplant. Another option for a free muscle transfer is the latissimus dorsi muscle. A disadvantage is that it can only be harvested with the patient in lateral decubitus or prone position. Therefore, the patient has to be turned during the operation. Advantages of the latissimus dorsi muscle are its reliable anatomy and relatively simple dissection. Analogue to the gracilis muscle, this muscle can be trimmed to the correct size and volume. The latissimus dorsi muscle is also a parallel-fibered muscle.[12] Its long neurovascular bundle makes a one-stage facial reanimation without a CFNG possible. By using the long thoracodorsal nerve of the latissimus dorsi muscle, direct coaptation to the facial nerve on the other side can be performed.[12]
The third option is the pectoralis minor muscle, which is mainly used in children. Advantages of this muscle are its relatively small size and flat and fan-like shape, obviating the need for trimming without bulkiness as a result.[7] In addition, the pectoralis minor muscle has a muscle fibre orientation that is much alike with the facial muscles.[12] However, as dissection of this muscle is rather difficult and the neurovascular anatomy is variable, nowadays surgeons tend to use it less frequently. Furthermore, the pectoralis minor muscle is not a parallel-fibered muscle, and it is oversized in adults.[7]
During a one-stage or two-stage CFNG procedure, one or more non-affected facial nerve branches are used for reinnervation of the paralysed side. In the one stage procedure a free muscle transplant with a latissimus dorsi graft or a nerve graft (using the sural nerve or saphenous nerve) can be used. The latissimus dorsi graft is used because of its long thoracodorsal nerve. Therefore, it can be coapted directly to the normal functioning facial nerve.[12] The one stage CFNG, implies an end-to-side coaptation of the sural or saphenous nerve to the distal end of the affected facial nerve.[6] In the two-stage procedure, an incision in front of the ear is made on the non-paralysed side. Upon electrical stimulation, the nerve which produces the best contraction of the zygomatic muscles (and so the appearance of a smile) is selected.[5] This branch is then sectioned. The sural or saphenous nerve as cross facial nerve graft is coapted to this unaffected branch of the facial nerve and tunnelled across the face to the paralysed side through a subcutaneous tunnel.[10] The end of the graft is positioned in front of the tragus (cartilage in front of the ear) on the paralysed side. Nine to twelve months is needed for axonal regeneration in the cross facial nerve graft, because the result of damaged nerve tissue is loss of structure and axonal function. Degeneration appears distally in the paralysed facial nerve but this takes time, this process is called Wallerian degeneration. During the second stage end-to-side or end-to-end nerve coaptation to the proximal end of the paralysed facial nerve is performed with a microscope.[5] And a free muscle transplant is placed, if indicated.[citation needed]
Likewise the "babysitter" procedure uses the CFNG, in combination with the masseteric or hypoglossal nerve. In the "babysitter" procedure, the hypoglossal nerve or masseteric nerve on the affected side is identified. This donor nerve is then attached to the distal end of the paralysed facial nerve.[5] Techniques for donor nerve transfers are transposition of the entire donor nerve, partial transposition by splitting the donor nerve longitudinally[2] or indirect hypoglossal- or masseteric-facial anatomosis using a 'jump' interposition graft.[8] This usually is the great auricular nerve or sural nerve. These hypoglossal- or masseteric-facial nerve anastomosis using a 'jump' interposition graft can be used to directly reinnervate the paralysed facial muscles or as a "babysitter" procedure. The goal of the latter is only to achieve fast reinnervation of the mimetic muscle to prevent irreversible atrophy. Simultaneously one or more CFNGs are performed to eventually reinnervate the mimetic muscles, again as a one- or two-stage procedure,[13] depending on the choice for the free muscle transfer graft. If a two-stage procedure is performed, the CFNGs are connected to the distal branches of the paralysed facial nerve during the second stage 9 to 12 months later. The donor nerve can be left intact. If a free muscle transfer is indicated, this is also performed in the second stage of the procedure to augment the partially reinnervated mimic muscles by the hypoglossal nerve.[10]
In case of longstanding facial paralysis with irreversible muscle atrophy and unavailability of a suitable donor facial nerve, a free muscle graft is indicated for smile restoration, which has to be reinnervated by another donor nerve (usually the masseteric nerve) in an end-to-end fashion. Through an incision in front of the ear, the cheek flap is elevated below the underlying layer of fat. Here the nerve stimulator can be used in identifying the donor motor nerve to the masseter muscle. Once the nerve is identified, it is dissected from its connections and traced into the muscle to free as much length as possible.[2]
Results
All procedures in general show an improvement of symmetry of smile and patient satisfaction, although time of recovery differs between different approaches. Primary neurorrhaphy provides the best possible outcome, as the anatomy and function of the damaged facial nerve is restored.[7][8] After primary neurorrhaphy of the facial nerve mean recovery time typically is 6 to 12 months.[9] The contraction amplitude after using a CFNG is usually not very powerful, but it results in a relatively spontaneous smile because the contralateral healthy facial nucleus controls the movements.[14] After a CFNG procedure the first signs of reinnervation usually occur between 4 and 12 months.[15] The use of the masseteric nerve provides an amount of movement that is within the normal range, resulting in a more symmetrical but not completely emotional smile.[14] Nerve transfers using the hypoglossal or masseteric nerves and the "babysitter" procedure result in first contractions of the mimic muscles after approximately 4 to 6 months.[4][5] However, after the use of the hypoglossal nerve control of facial movements is hard to obtain by the patient and a spontaneous smile may not occur at all.[5]
True spontaneity of a smile will not occur at the same rate in all dynamic smile reconstructions. A spontaneous smile is smiling without consciously thinking about it.[14] The primary neurorrhaphy and free muscle transfer are the only options to restore a true spontaneous smile.[7][13] Although the masseteric nerve transfer provides a strong smile within the range of normal, it never becomes truly spontaneous and emotional.[14] But with practice, the majority of patients can provide a spontaneous smile some of the time[14] due to the plasticity of the cerebral cortex.[13] Effective rehabilitation can also prevent biting whilst smiling, when using the masseteric nerve as nerve transfer.[14]
Complications
There are several complications, however, most patients find them less invalidating than the inability to smile.[14] General postoperative complications are infection of the muscle donor site,[15] facial abscess, hypertrophic scars,[3]hematoma,[15] and swelling of the face or muscle donor site.[14] In some cases of incomplete facial paralysis, the procedure had a decline in function as a result. However, this improved after only a few months.[15] Almost all procedures show synkinesis, meaning involuntary movements appear during the voluntary movements. In primary neurorrhapy, with or without an interposition graft, perineural fibrosis is a common complication.[8] With the use of the CFNG there is a risk of sensory deficits in the lower part of the leg, due to the sural or sapheneous nerve graft.[2] A complication seen with the use of the masseteric nerve is the inability to chew without the appearance of a smile.[14] The hypoglossal nerve as a donor nerve can induce tongue atrophy due to denervation.[5]
Related Research Articles
Breast reconstruction is the surgical process of rebuilding the shape and look of a breast, most commonly in women who have had surgery to treat breast cancer. It involves using autologous tissue, prosthetic implants, or a combination of both with the goal of reconstructing a natural-looking breast. This process often also includes the rebuilding of the nipple and areola, known as nipple-areola complex (NAC) reconstruction, as one of the final stages.
The latissimus dorsi is a large, flat muscle on the back that stretches to the sides, behind the arm, and is partly covered by the trapezius on the back near the midline. The word latissimus dorsi comes from Latin and means "broadest [muscle] of the back", from "latissimus" ' and "dorsum". The pair of muscles are commonly known as "lats", especially among bodybuilders. The latissimus dorsi is the largest muscle in the upper body.
Möbius syndrome or Moebius syndrome is a rare congenital neurological disorder which is characterized by facial paralysis and the inability to move the eyes from side to side. Most people with Möbius syndrome are born with complete facial paralysis and cannot close their eyes or form facial expressions. Limb and chest wall abnormalities sometimes occur with the syndrome. People with Möbius syndrome have normal intelligence, although their lack of facial expression is sometimes incorrectly taken to be due to dullness or unfriendliness. It is named for Paul Julius Möbius, a German neurologist who first described the syndrome in 1888. In 1994, the "Moebius Syndrome Foundation" was founded, and later that year the first "Moebius Syndrome Foundation Conference" was held in Los Angeles.
Rhinoplasty, commonly called nose job, medically called nasal reconstruction is a plastic surgery procedure for altering and reconstructing the nose. There are two types of plastic surgery used – reconstructive surgery that restores the form and functions of the nose and cosmetic surgery that changes the appearance of the nose. Reconstructive surgery seeks to resolve nasal injuries caused by various traumas including blunt, and penetrating trauma and trauma caused by blast injury. Reconstructive surgery can also treat birth defects, breathing problems, and failed primary rhinoplasties. Rhinoplasty may remove a bump, narrow nostril width, change the angle between the nose and the mouth, or address injuries, birth defects, or other problems that affect breathing, such as a deviated nasal septum or a sinus condition. Surgery only on the septum is called a septoplasty.
Grafting refers to a surgical procedure to move tissue from one site to another on the body, or from another creature, without bringing its own blood supply with it. Instead, a new blood supply grows in after it is placed. A similar technique where tissue is transferred with the blood supply intact is called a flap. In some instances, a graft can be an artificially manufactured device. Examples of this are a tube to carry blood flow across a defect or from an artery to a vein for use in hemodialysis.
Facial nerve paralysis is a common problem that involves the paralysis of any structures innervated by the facial nerve. The pathway of the facial nerve is long and relatively convoluted, so there are a number of causes that may result in facial nerve paralysis. The most common is Bell's palsy, a disease of unknown cause that may only be diagnosed by exclusion of identifiable serious causes.
Microsurgery is a general term for surgery requiring an operating microscope. The most obvious developments have been procedures developed to allow anastomosis of successively smaller blood vessels and nerves which have allowed transfer of tissue from one part of the body to another and re-attachment of severed parts. Microsurgical techniques are utilized by several specialties today, such as general surgery, ophthalmology, orthopedic surgery, gynecological surgery, otolaryngology, neurosurgery, oral and maxillofacial surgery, plastic surgery, podiatric surgery and pediatric surgery.
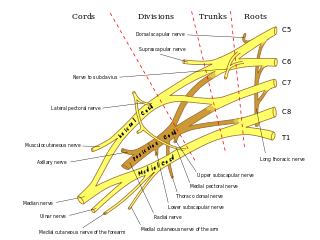
Erb's palsy is a paralysis of the arm caused by injury to the upper group of the arm's main nerves, specifically the severing of the upper trunk C5–C6 nerves. These form part of the brachial plexus, comprising the ventral rami of spinal nerves C5–C8 and thoracic nerve T1. These injuries arise most commonly, but not exclusively, from shoulder dystocia during a difficult birth. Depending on the nature of the damage, the paralysis can either resolve on its own over a period of months, necessitate rehabilitative therapy, or require surgery.
Hypertelorism is an abnormally increased distance between two organs or bodily parts, usually referring to an increased distance between the orbits (eyes), or orbital hypertelorism. In this condition the distance between the inner eye corners as well as the distance between the pupils is greater than normal. Hypertelorism should not be confused with telecanthus, in which the distance between the inner eye corners is increased but the distances between the outer eye corners and the pupils remain unchanged.
Fazio–Londe disease (FLD), also called progressive bulbar palsy of childhood, is a very rare inherited motor neuron disease of children and young adults and is characterized by progressive paralysis of muscles innervated by cranial nerves. FLD, along with Brown–Vialetto–Van Laere syndrome (BVVL), are the two forms of infantile progressive bulbar palsy, a type of progressive bulbar palsy in children.
A traumatic neuroma is a type of neuroma which results from trauma to a nerve, usually during a surgical procedure. The most common oral locations are on the tongue and near the mental foramen of the mouth. They are relatively rare on the head and neck.
Synkinesis is a neurological symptom in which a voluntary muscle movement causes the simultaneous involuntary contraction of other muscles. An example might be smiling inducing an involuntary contraction of the eye muscles, causing a person to squint when smiling. Facial and extraocular muscles are affected most often; in rare cases, a person's hands might perform mirror movements.
Jaw reduction or mandible angle reduction is a type of surgery to narrow the lower one-third of the face—particularly the contribution from the mandible and its muscular attachments. There are several techniques for treatment—including surgical and non-surgical methods. A square lower jaw can be considered a masculine trait, especially in Asian countries. As a result, whereas square lower jaws are often considered a positive trait in men, a wide mandible can be perceived as discordant or masculine on women, or sometimes in certain men, particularly when there is asymmetry.
A DIEP flap is type of breast reconstruction where blood vessels, fat, and skin from the lower belly are relocated to the chest to rebuild breasts after mastectomy. DIEP stands for the deep inferior epigastric perforator artery, which runs through the abdomen. This is a type of autologous reconstruction, meaning one's own tissue is used.
Bone segment navigation is a surgical method used to find the anatomical position of displaced bone fragments in fractures, or to position surgically created fragments in craniofacial surgery. Such fragments are later fixed in position by osteosynthesis. It has been developed for use in craniofacial and oral and maxillofacial surgery.
Nasal reconstruction using a paramedian forehead flap within oral and maxillofacial surgery, is a surgical technique to reconstruct different kinds of nasal defects. In this operation a reconstructive surgeon uses skin from the forehead above the eyebrow and pivots it vertically to replace missing nasal tissue. Throughout history the technique has been modified and adjusted by many different surgeons and it has evolved to become a popular way of repairing nasal defects.
The tint of forehead skin so exactly matches that of the face and nose that it must be first choice. Is not the forehead the crowning feature of the face and important in expression? Why then should we jeopardize its beauty to make a nose? First, because in many instances, the forehead makes far and away the best nose. Second, with some plastic juggling, the forehead defect can be camouflaged effectively.
Flap surgery is a technique in plastic and reconstructive surgery where any type of tissue is lifted from a donor site and moved to a recipient site with an intact blood supply. This is distinct from a graft, which does not have an intact blood supply and therefore relies on growth of new blood vessels. This is done to fill a defect such as a wound resulting from injury or surgery when the remaining tissue is unable to support a graft, or to rebuild more complex anatomic structures such as breast or jaw.
Perforator flap surgery is a technique used in reconstructive surgery where skin and/or subcutaneous fat are removed from a distant or adjacent part of the body to reconstruct the excised part. The vessels that supply blood to the flap are isolated perforator(s) derived from a deep vascular system through the underlying muscle or intermuscular septa. Some perforators can have a mixed septal and intramuscular course before reaching the skin. The name of the particular flap is retrieved from its perforator and not from the underlying muscle. If there is a potential to harvest multiple perforator flaps from one vessel, the name of each flap is based on its anatomical region or muscle. For example, a perforator that only traverses through the septum to supply the underlying skin is called a septal perforator. Whereas a flap that is vascularised by a perforator traversing only through muscle to supply the underlying skin is called a muscle perforator. According to the distinct origin of their vascular supply, perforators can be classified into direct and indirect perforators. Direct perforators only pierce the deep fascia, they don't traverse any other structural tissue. Indirect perforators first run through other structures before piercing the deep fascia.
Free-flap breast reconstruction is a type of autologous-tissue breast reconstruction applied after mastectomy for breast cancer, without the emplacement of a breast implant prosthesis. As a type of plastic surgery, the free-flap procedure for breast reconstruction employs tissues, harvested from another part of the woman's body, to create a vascularised flap, which is equipped with its own blood vessels. Breast-reconstruction mammoplasty can sometimes be realised with the application of a pedicled flap of tissue that has been harvested from the latissimus dorsi muscle, which is the broadest muscle of the back, to which the pedicle (“foot”) of the tissue flap remains attached until it successfully grafts to the recipient site, the mastectomy wound. Moreover, if the volume of breast-tissue excised was of relatively small mass, breast augmentation procedures, such as autologous-fat grafting, also can be applied to reconstruct the breast lost to mastectomy.
Nerve allotransplantation is the transplantation of a nerve to a receiver from a donor of the same species. For example, nerve tissue is transplanted from one person to another. Allotransplantation is a commonly used type of transplantation of which nerve repair is one specific aspect.
1 2 O'Brien BM, Pederson WC, Khazanchi RK, Morrison WA, MacLeod AM, Kumar V (July 1990). "Results of management of facial palsy with microvascular free-muscle transfer". Plast. Reconstr. Surg. 86 (1): 12–22, discussion 23–4. doi:10.1097/00006534-199007000-00002. PMID2359779. S2CID25457239.
1 2 3 4 5 Harii K, Asato H, Yoshimura K, Sugawara Y, Nakatsuka T, Ueda K (September 1998). "One-stage transfer of the latissimus dorsi muscle for reanimation of a paralyzed face: a new alternative". Plast. Reconstr. Surg. 102 (4): 941–51. doi:10.1097/00006534-199809040-00001. PMID9734407.
1 2 3 Watanabe Y, Akizuki T, Ozawa T, Yoshimura K, Agawa K, Ota T (December 2009). "Dual innervation method using one-stage reconstruction with free latissimus dorsi muscle transfer for re-animation of established facial paralysis: simultaneous reinnervation of the ipsilateral masseter motor nerve and the contralateral facial nerve to improve the quality of smile and emotional facial expressions". J Plast Reconstr Aesthet Surg. 62 (12): 1589–97. doi:10.1016/j.bjps.2008.07.025. PMID19010754.
1 2 3 4 5 6 7 8 9 Manktelow RT, Tomat LR, Zuker RM, Chang M (September 2006). "Smile reconstruction in adults with free muscle transfer innervated by the masseter motor nerve: effectiveness and cerebral adaptation". Plast. Reconstr. Surg. 118 (4): 885–99. doi:10.1097/01.prs.0000232195.20293.bd. PMID16980848. S2CID24119304.
1 2 3 4 Takushima A, Harii K, Okazaki M, Ohura N, Asato H (April 2009). "Availability of latissimus dorsi minigraft in smile reconstruction for incomplete facial paralysis: quantitative assessment based on the optical flow method". Plast. Reconstr. Surg. 123 (4): 1198–208. doi:10.1097/PRS.0b013e31819e2606. PMID19337088. S2CID1247404.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.