| Accessory nerve | |
|---|---|
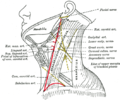
 View of the human brain from below. The accessory nerve emerges from the medulla of the brainstem, and is visible at the bottom of the image in blue. | |
| Details | |
| Innervates | Sternocleidomastoid muscle, trapezius muscle |
| Identifiers | |
| Latin | nervus accessorius |
| MeSH | D000055 |
| TA98 | A14.2.01.184 A14.1.02.112 |
| TA2 | 6352 |
| FMA | 6720 |
| Anatomical terms of neuroanatomy | |
| Cranial nerves |
|---|
|
The accessory nerve, also known as the eleventh cranial nerve, cranial nerve XI, or simply CN XI, is a cranial nerve that supplies the sternocleidomastoid and trapezius muscles. It is classified as the eleventh of twelve pairs of cranial nerves because part of it was formerly believed to originate in the brain. The sternocleidomastoid muscle tilts and rotates the head, whereas the trapezius muscle, connecting to the scapula, acts to shrug the shoulder.
Contents
- Structure
- Nucleus
- Variation
- Development
- Function
- Classification
- Clinical significance
- Examination
- Injury
- History
- See also
- Additional images
- References
- External links
Traditional descriptions of the accessory nerve divide it into a spinal part and a cranial part. [1] The cranial component rapidly joins the vagus nerve, and there is ongoing debate about whether the cranial part should be considered part of the accessory nerve proper. [2] [1] Consequently, the term "accessory nerve" usually refers only to nerve supplying the sternocleidomastoid and trapezius muscles, also called the spinal accessory nerve. [3]
Strength testing of these muscles can be measured during a neurological examination to assess function of the spinal accessory nerve. Poor strength or limited movement are suggestive of damage, which can result from a variety of causes. Injury to the spinal accessory nerve is most commonly caused by medical procedures that involve the head and neck. [4] Injury can cause wasting of the shoulder muscles, winging of the scapula, and weakness of shoulder abduction and external rotation. [5]
The accessory nerve is derived from the basal plate of the embryonic spinal segments C1–C6. [6]



{kind=link}