| Lingual nerve | |
|---|---|
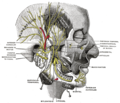
 Distribution of the maxillary and mandibular nerves, and the submaxillary ganglion. | |
 The mouth cavity. The apex of the tongue is turned upward, and on the right side a superficial dissection of its under surface has been made. | |
| Details | |
| From | Mandibular nerve |
| Innervates | Tongue |
| Identifiers | |
| Latin | nervus lingualis |
| MeSH | D008036 |
| TA98 | A14.2.01.081 |
| TA2 | 6267 |
| FMA | 53218 |
| Anatomical terms of neuroanatomy | |
The lingual nerve carries sensory innervation from the anterior two-thirds of the tongue. It contains fibres from both the mandibular division of the trigeminal nerve (CN V3) and from the facial nerve (CN VII). The fibres from the trigeminal nerve are for touch, pain and temperature (general sensation), and the ones from the facial nerve are for taste (special sensation).









{kind=link}
{kind=link}