Physiology
Vagal maneuvers serve to stimulate the vagus nerve (cranial nerve X) through various mechanisms. The longest nerve in the body, the vagus nerve serves both motor and sensory functions through afferent and efferent signaling to and from the brain. The vagus nerve releases the neurotransmitter acetylcholine, [13] and is a main mediator for the parasympathetic nervous system.
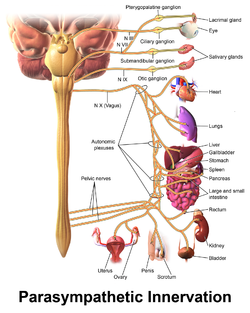
The vagus nerve exits the skull through the jugular foramen, moving down through the carotid sheath and dividing many times to influence multiple organ systems and directly innervating the pharynx, larynx, esophagus, heart, lung, and GI tract. Due to this wide nerve distribution, many physiologic process may be influenced through its stimulation, including heart rate and blood pressure. [14]
Stimulation of the vagus nerve through vagal maneuvers is thought to effect afferent fibers that carry sensory information from its distribution throughout the body to the nucleus tractus solitarii (NTS) in the dorsal medullary complex, where it is then relayed to other areas of the brain. This stimulation can also be done more directly through a therapy called vagus nerve stimulation (VNS), which utilizes an implanted neuro-stimulator device and is approved clinically for controlling seizures in epilepsy patients and drug resistant depression. [15]
Vagal maneuvers make use of the vagus nerve's afferent and efferent bifunctional role, triggering reflexes (like the baroreceptor reflex, chemoreceptor reflex) and utilizing those afferent nerve fibers to increase nerve activity. This results in increased parasympathetic signaling through its efferent distribution and is mediated by the chemical messenger acetylcholine. [4]