Heparin-induced thrombocytopenia (HIT) is the development of thrombocytopenia (a low platelet count), due to the administration of various forms of heparin, an anticoagulant. HIT predisposes to thrombosis (the abnormal formation of blood clots inside a blood vessel). When thrombosis is identified the condition is called heparin-induced thrombocytopenia and thrombosis (HITT). HIT is caused by the formation of abnormal antibodies that activate platelets, which release microparticles that activate thrombin, leading to thrombosis. If someone receiving heparin develops new or worsening thrombosis, or if the platelet count falls, HIT can be confirmed with specific blood tests.[1]
The treatment of HIT requires stopping heparin treatment, and both protection from thrombosis and choice of an agent that will not reduce the platelet count any further. Several alternatives are available for this purpose; mainly used are danaparoid, fondaparinux, argatroban, and bivalirudin.[2][3]
While heparin was discovered in the 1930s, HIT was not reported until the 1960s.[4]
Signs and symptoms
Heparin may be used for both prevention and the treatment of thrombosis. It exists in two main forms: an "unfractionated" form that can be injected under the skin (subcutaneously) or through an intravenous infusion, and a "low molecular weight" form that is generally given subcutaneously. Commonly used low molecular weight heparins are enoxaparin, dalteparin, nadroparin and tinzaparin.[5][6]
In HIT, the platelet count in the blood falls below the normal range, a condition called thrombocytopenia. However, it is generally not low enough to lead to an increased risk of bleeding. Most people with HIT, therefore, do not experience any symptoms. Typically, the platelet count falls 5–14 days after heparin is first given; if someone has received heparin in the previous three months, the fall in platelet count may occur sooner, sometimes within a day.[1]
The most common symptom of HIT is enlargement or extension of a previously diagnosed blood clot, or the development of a new blood clot elsewhere in the body. This may take the form of clots either in arteries or veins, causing arterial or venous thrombosis, respectively. Examples of arterial thrombosis are stroke, myocardial infarction ("heart attack"), and acute leg ischemia. Venous thrombosis may occur in the leg or arm in the form of deep vein thrombosis (DVT) and in the lung in the form of a pulmonary embolism (PE); the latter usually originates in the leg, but migrates to the lung.[1][7]
The administration of heparin can cause the development of HIT antibodies, suggesting heparin may act as a hapten, thus may be targeted by the immune system. In HIT, the immune system forms antibodies against heparin when it is bound to a protein called platelet factor 4 (PF4). These antibodies are usually of the IgG class and their development usually takes about five days. However, those who have been exposed to heparin in the last few months may still have circulating IgG, as IgG-type antibodies generally continue to be produced even when their precipitant has been removed. This is similar to immunity against certain microorganisms, with the difference that the HIT antibody does not persist more than three months.[1][7] HIT antibodies have been found in individuals with thrombocytopenia and thrombosis who had no prior exposure to heparin, but the majority are found in people who are receiving heparin.[8]
The IgG antibodies form a complex with heparin and PF4 in the bloodstream. The tail of the antibody then binds to the FcγIIa receptor, a protein on the surface of the platelet. This results in platelet activation and the formation of platelet microparticles, which initiate the formation of blood clots; the platelet count falls as a result, leading to thrombocytopenia.[1][7] In addition, the reticuloendothelial system (mostly the spleen) removes the antibody-coated platelets, further contributing to the thrombocytopenia.
Formation of PF4-heparin antibodies is common in people receiving heparin, but only a proportion of these develop thrombocytopenia or thrombosis.[1] This has been referred to as an "iceberg phenomenon".[4]
Diagnosis
HIT may be suspected if blood tests show a falling platelet count in someone receiving heparin, even if the heparin has already been discontinued. Professional guidelines recommend that people receiving heparin have a complete blood count (which includes a platelet count) on a regular basis while receiving heparin.[5][9]
However, not all people with a falling platelet count while receiving heparin turn out to have HIT. The timing, severity of the thrombocytopenia, the occurrence of new thrombosis, and the presence of alternative explanations, all determine the likelihood that HIT is present. A commonly used score to predict the likelihood of HIT is the "4 Ts" score introduced in 2003.[10] A score of 0–8 points is generated; if the score is 0–3, HIT is unlikely. A score of 4–5 indicates intermediate probability, while a score of 6–8 makes it highly likely. Those with a high score may need to be treated with an alternative drug, while more sensitive and specific tests for HIT are performed, while those with a low score can safely continue receiving heparin, as the likelihood that they have HIT is extremely low.[1][7][11] In an analysis of the reliability of the 4T score, a low score had a negative predictive value of 0.998, while an intermediate score had a positive predictive value of 0.14 and a high score a positive predictive value of 0.64; intermediate and high scores, therefore, warrant further investigation.[12]
Element
The 4T score for heparin-induced thrombocytopenia[9][10]
Thrombocytopenia
2 points if the fall in platelet count is >50% of the previous value, AND the lowest count (nadir) is 20–100×109/liter 1 point if the fall is 30–50% or the nadir is 10–19×109/liter No points if the fall is less than 30% or the nadir is <10×109/liter.
Timing
2 points if the fall is between days 5–10 after commencement of treatment 1 point if the fall is after day 10. If someone has been exposed to heparin within the last 30 days and then has a drop in platelet count within a day of reexposure, 2 points are given. If the previous exposure was 30–100 days ago, 1 point If the fall is early but there has been no previous heparin exposure, no points.
Thrombosis
2 points in new proven thrombosis, skin necrosis (see below), or systemic reaction 1 point if progressive or recurrent thrombosis, silent thrombosis or red skin lesions No points if there are no symptoms.
Alternative cause possible
2 points if no other cause 1 point if there is a possible alternative cause No points if there is a definite alternative cause.
The first screening test in someone suspected of having HIT is aimed at detecting antibodies against heparin-PF4 complexes. This may be with a laboratory test of the enzyme-linked immunosorbent assay type. This ELISA test, however, detects all circulating antibodies that bind heparin-PF4 complexes, and may also falsely identify antibodies that do not cause HIT. Therefore, those with a positive ELISA are tested further with a functional assay. This test uses platelets and serum from the patient; the platelets are washed and mixed with serum and heparin. The sample is then tested for the release of serotonin, a marker of platelet activation. If this serotonin release assay (SRA) shows high serotonin release, the diagnosis of HIT is confirmed. The SRA test is difficult to perform and is usually only done in regional laboratories.[1][7]
If someone has been diagnosed with HIT, some recommend routine Doppler sonography of the leg veins to identify deep vein thromboses, as this is very common in HIT.[7][11]
Treatment
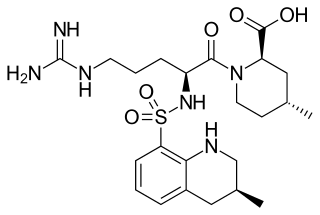
Molecular structure of argatroban, a direct thrombin inhibitor used as an alternative to heparin in HIT
Given the fact that HIT predisposes strongly to new episodes of thrombosis, simply discontinuing the heparin administration is insufficient. Generally, an alternative anticoagulant is needed to suppress the thrombotic tendency while the generation of antibodies stops and the platelet count recovers. To make matters more complicated, the other most commonly used anticoagulant, warfarin, should not be used in HIT until the platelet count is at least 150×109/L because a very high risk of warfarin necrosis exists in people with HIT who have low platelet counts. Warfarin necrosis is the development of skin gangrene in those receiving warfarin or a similar vitamin K inhibitor. If the patient was receiving warfarin at the time when HIT is diagnosed, the activity of warfarin is reversed with vitamin K.[1][9] Transfusing platelets is discouraged, as a theoretical risk indicates that this may worsen the risk of thrombosis; the platelet count is rarely low enough to be the principal cause of significant hemorrhage.[9]
Various nonheparin agents are used as alternatives to heparin therapy to provide anticoagulation in those with strongly suspected or proven HIT: danaparoid, fondaparinux, bivalirudin, and argatroban.[2][3] Not all agents are available in all countries, and not all are approved for this specific use. For instance, argatroban is only recently licensed in the United Kingdom, and danaparoid is not available in the United States.[8] Fondaparinux, a factor Xa inhibitor, is commonly used off label for HIT treatment in the United States.[citation needed]
According to a systematic review, people with HIT treated with lepirudin showed a relative risk reduction of clinical outcome (death, amputation, etc.) to be 0.52 and 0.42 when compared to patient controls. In addition, people treated with argatroban for HIT showed a relative risk reduction of the above clinical outcomes to be 0.20 and 0.18.[13] Lepirudin production stopped on May 31, 2012.[14]
Epidemiology
Up to 8% of patients receiving heparin are at risk to develop HIT antibodies, but only 1–5% on heparin will progress to develop HIT with thrombocytopenia and subsequently one-third of them may develop arterial or venous thrombosis.[1] After vascular surgery, 34% of patients receiving heparin developed HIT antibodies without clinical symptoms.[15] The exact number of cases of HIT in the general population is unknown. What is known is that women receiving heparin after a recent surgical procedure, particularly cardiothoracic surgery, have a higher risk, while the risk is very low in women just before and after giving birth. Some studies have shown that HIT is less common in those receiving low molecular weight heparin.[7]
History
While heparin was introduced for clinical use in the late 1930s, new thrombosis in people treated with heparin was not described until 1957, when vascular surgeons reported the association.[4][16] The fact that this phenomenon occurred together with thrombocytopenia was reported in 1969;[17] prior to this time, platelet counts were not routinely performed.[4] A 1973 report established HIT as a diagnosis, as well as suggesting that its features were the result of an immune process.[4][18]
Initially, various theories existed about the exact cause of the low platelets in HIT. Gradually, evidence accumulated on the exact underlying mechanism.[4] In 1984–1986, John G. Kelton and colleagues at McMaster University Medical School developed the laboratory tests that could be used to confirm or exclude heparin-induced thrombocytopenia.[4][19]
Treatment was initially limited to aspirin and warfarin, but the 1990s saw the introduction of a number of agents that could provide anticoagulation without a risk of recurrent HIT.[4] Older terminology distinguishes between two forms of heparin-induced thrombocytopenia: type 1 (mild, nonimmune mediated and self-limiting fall in platelet count) and type 2, the form described above. Currently, the term HIT is used without a modifier to describe the immune-mediated severe form.[4]
An anticoagulant, commonly known as a blood thinner, is a chemical substance that prevents or reduces coagulation of blood, prolonging the clotting time. Some of them occur naturally in blood-eating animals such as leeches and mosquitoes, where they help keep the bite area unclotted long enough for the animal to obtain some blood.
Warfarin is an anticoagulant used as a medication under several brand names including Coumadin. While the drug is described as a "blood thinner", it does not reduce viscosity but rather inhibits coagulation. Accordingly, it is commonly used to prevent blood clots in the circulatory system such as deep vein thrombosis and pulmonary embolism, and to protect against stroke in people who have atrial fibrillation, valvular heart disease, or artificial heart valves. Less commonly, it is used following ST-segment elevation myocardial infarction and orthopedic surgery. It is usually taken by mouth, but may also be administered intravenously.
Heparin, also known as unfractionated heparin (UFH), is a medication and naturally occurring glycosaminoglycan. Since heparins depend on the activity of antithrombin, they are considered anticoagulants. Specifically it is also used in the treatment of heart attacks and unstable angina. It is given intravenously or by injection under the skin. Other uses for its anticoagulant properties include inside blood specimen test tubes and kidney dialysis machines.
Antiphospholipid syndrome, or antiphospholipid antibody syndrome, is an autoimmune, hypercoagulable state caused by antiphospholipid antibodies. APS can lead to blood clots (thrombosis) in both arteries and veins, pregnancy-related complications, and other symptoms like low platelets, kidney disease, heart disease, and rash. Although the exact etiology of APS is still not clear, genetics is believed to play a key role in the development of the disease. Diagnosis is made based on symptoms and testing, but sometimes research criteria are used to aid in diagnosis. The research criteria for definite APS requires one clinical event and two positive blood test results spaced at least three months apart that detect lupus anticoagulant, anti-apolipoprotein antibodies, and/or anti-cardiolipin antibodies.
Immune thrombocytopenic purpura (ITP), also known as idiopathic thrombocytopenic purpura or immune thrombocytopenia, is a type of thrombocytopenic purpura characterized by a low platelet count in the absence of other causes, and accompanied by a red-purple rash called purpura. It leads to an increased risk of bleeding. ITP manifests in two distinct clinical syndromes: an acute form observed in children, and chronic conditions observed in adults. The acute form often follows an infection and typically resolves within two months, while chronic immune thrombocytopenia persists for longer than six months and its specific cause is unknown.
In hematology, thrombocytopenia is a condition characterized by abnormally low levels of platelets in the blood. Low levels of platelets in turn may lead to prolonged or excessive bleeding. It is the most common coagulation disorder among intensive care patients and is seen in a fifth of medical patients and a third of surgical patients.
Deep vein thrombosis (DVT) is a type of venous thrombosis involving the formation of a blood clot in a deep vein, most commonly in the legs or pelvis. A minority of DVTs occur in the arms. Symptoms can include pain, swelling, redness, and enlarged veins in the affected area, but some DVTs have no symptoms.
Low-molecular-weight heparin (LMWH) is a class of anticoagulant medications. They are used in the prevention of blood clots and treatment of venous thromboembolism and in the treatment of myocardial infarction.
Thrombophilia is an abnormality of blood coagulation that increases the risk of thrombosis. Such abnormalities can be identified in 50% of people who have an episode of thrombosis that was not provoked by other causes. A significant proportion of the population has a detectable thrombophilic abnormality, but most of these develop thrombosis only in the presence of an additional risk factor.
Argatroban is an anticoagulant that is a small molecule direct thrombin inhibitor. In 2000, argatroban was licensed by the Food and Drug Administration (FDA) for prophylaxis or treatment of thrombosis in patients with heparin-induced thrombocytopenia (HIT). In 2002, it was approved for use during percutaneous coronary interventions in patients who have HIT or are at risk for developing it. In 2012, it was approved by the MHRA in the UK for anticoagulation in patients with heparin-induced thrombocytopenia Type II (HIT) who require parenteral antithrombotic therapy.
Dilute Russell's viper venom time (dRVVT) is a laboratory test often used for detection of lupus anticoagulant (LA).
Renal vein thrombosis (RVT) is the formation of a clot in the vein that drains blood from the kidneys, ultimately leading to a reduction in the drainage of one or both kidneys and the possible migration of the clot to other parts of the body. First described by German pathologist Friedrich Daniel von Recklinghausen in 1861, RVT most commonly affects two subpopulations: newly born infants with blood clotting abnormalities or dehydration and adults with nephrotic syndrome.
Danaparoid sodium (Orgaran) is an anticoagulant with an antithrombotic action due to inhibition of thrombin generation (TGI) by two mechanisms: indirect inactivation of Factor Xa via AT and direct inhibition of thrombin activation of Factor IX. It also possesses a minor anti-thrombin activity, mediated equally via AT and Heparin Co-factor II producing a ratio of anti-Xa:IIa activity >22. [Meuleman DG. Haemostasis 1992;22:58-65 and Ofosu FA Haemostasis 1992;22:66-72]
Platelet factor 4 (PF4) is a small cytokine belonging to the CXC chemokine family that is also known as chemokine ligand 4 (CXCL4). This chemokine is released from alpha-granules of activated platelets during platelet aggregation, and promotes blood coagulation by moderating the effects of heparin-like molecules. Due to these roles, it is predicted to play a role in wound repair and inflammation. It is usually found in a complex with proteoglycan.
Ancrod is a defibrinogenating agent derived from the venom of the Malayan pit viper. Defibrinogenating blood produces an anticoagulant effect. Ancrod is not approved or marketed in any country. It is a thrombin-like serine protease.
Direct thrombin inhibitors (DTIs) are a class of medication that act as anticoagulants by directly inhibiting the enzyme thrombin. Some are in clinical use, while others are undergoing clinical development. Several members of the class are expected to replace heparin and warfarin in various clinical scenarios.
Hypercoagulability in pregnancy is the propensity of pregnant women to develop thrombosis. Pregnancy itself is a factor of hypercoagulability, as a physiologically adaptive mechanism to prevent post partum bleeding. However, when combined with an additional underlying hypercoagulable states, the risk of thrombosis or embolism may become substantial.
Cerebral venous sinus thrombosis (CVST), cerebral venous and sinus thrombosis or cerebral venous thrombosis (CVT), is the presence of a blood clot in the dural venous sinuses, the cerebral veins, or both. Symptoms may include severe headache, visual symptoms, any of the symptoms of stroke such as weakness of the face and limbs on one side of the body, and seizures, which occur in around 40% of patients.
Direct thrombin inhibitors (DTIs) are a class of anticoagulant drugs that can be used to prevent and treat embolisms and blood clots caused by various diseases. They inhibit thrombin, a serine protease which affects the coagulation cascade in many ways. DTIs have undergone rapid development since the 90's. With technological advances in genetic engineering the production of recombinant hirudin was made possible which opened the door to this new group of drugs. Before the use of DTIs the therapy and prophylaxis for anticoagulation had stayed the same for over 50 years with the use of heparin derivatives and warfarin which have some well known disadvantages. DTIs are still under development, but the research focus has shifted towards factor Xa inhibitors, or even dual thrombin and fXa inhibitors that have a broader mechanism of action by both inhibiting factor IIa (thrombin) and Xa. A recent review of patents and literature on thrombin inhibitors has demonstrated that the development of allosteric and multi-mechanism inhibitors might lead the way to a safer anticoagulant.
Post-vaccination embolic and thrombotic events, termed vaccine-induced immune thrombotic thrombocytopenia (VITT), vaccine-induced prothrombotic immune thrombocytopenia (VIPIT), thrombosis with thrombocytopenia syndrome (TTS), vaccine-induced immune thrombocytopenia and thrombosis (VITT), or vaccine-associated thrombotic thrombocytopenia (VATT), are rare types of blood clotting syndromes that were initially observed in a number of people who had previously received the Oxford–AstraZeneca COVID‑19 vaccine (AZD1222) during the COVID‑19 pandemic. It was subsequently also described in the Janssen COVID‑19 vaccine, leading to the suspension of its use until its safety had been reassessed. On 5 May 2022 the FDA posted a bulletin limiting the use of the Janssen Vaccine to very specific cases due to further reassessment of the risks of TTS, although the FDA also stated in the same bulletin that the benefits of the vaccine outweigh the risks.
1 2 Watson, H (2012). "Guidelines on the diagnosis and management of heparin-induced thrombocytopenia: second edition". British Journal of Haematology. 159 (5): 528–40. doi:10.1111/bjh.12059. PMID23043677. S2CID5104368.
1 2 Hirsh J, Bauer KA, Donati MB, Gould M, Samama MM, Weitz JI (June 2008). "Parenteral anticoagulants: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition)". Chest. 133 (6 Suppl): 141S–159S. doi:10.1378/chest.08-0689. PMID18574264.
↑ Dooley C, Kaur R, Sobieraj DM (2014). "Comparison of the efficacy and safety of low molecular weight heparins for venous thromboembolism prophylaxis in medically ill patients". Curr Med Res Opin. 30 (3): 367–80. doi:10.1185/03007995.2013.837818. PMID23971722. S2CID206967565.
↑ Lindhoff-Last E, Eichler P, Stein M, Plagemann J, Gerdsen F, Wagner R, Ehrly AM, Bauersachs R (March 2000). "A prospective study on the incidence and clinical relevance of heparin-induced antibodies in patients after vascular surgery". Thromb. Res. 97 (6): 387–93. doi:10.1016/s0049-3848(99)00198-x. PMID10704647.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.