| Saphenous nerve | |
|---|---|
 Nerves of the right lower extremity. Front view. (Saphenous labeled at center right.) | |
| Details | |
| From | Femoral nerve (L3, L4) |
| Identifiers | |
| Latin | nervus saphenus |
| TA98 | A14.2.07.023 |
| TA2 | 6525 |
| FMA | 45262 |
| Anatomical terms of neuroanatomy | |
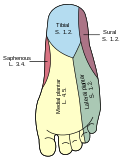
The saphenous nerve (long or internal saphenous nerve) is the largest cutaneous branch of the femoral nerve. It is derived from the lumbar plexus (L3-L4). It is a strictly sensory nerve, and has no motor function. It commences in the proximal (upper) thigh and travels along the adductor canal. Upon exiting the adductor canal, the saphenous nerve terminates by splitting into two terminal branches: the sartorial nerve, and the infrapatellar nerve (which together innervate the medial, anteromedial, posteromedial aspects of the distal thigh). The saphenous nerve is responsible for providing sensory innervation to the skin of the anteromedial leg. [1]