In humans and other primates, the knee joins the thigh with the leg and consists of two joints: one between the femur and tibia, and one between the femur and patella. It is the largest joint in the human body. The knee is a modified hinge joint, which permits flexion and extension as well as slight internal and external rotation. The knee is vulnerable to injury and to the development of osteoarthritis.

The posterior cruciate ligament (PCL) is a ligament in each knee of humans and various other animals. It works as a counterpart to the anterior cruciate ligament (ACL). It connects the posterior intercondylar area of the tibia to the medial condyle of the femur. This configuration allows the PCL to resist forces pushing the tibia posteriorly relative to the femur.
The anterior cruciate ligament (ACL) is one of a pair of cruciate ligaments in the human knee. The two ligaments are also called "cruciform" ligaments, as they are arranged in a crossed formation. In the quadruped stifle joint, based on its anatomical position, it is also referred to as the cranial cruciate ligament. The term cruciate translates to cross. This name is fitting because the ACL crosses the posterior cruciate ligament to form an “X”. It is composed of strong, fibrous material and assists in controlling excessive motion. This is done by limiting mobility of the joint. The anterior cruciate ligament is one of the four main ligaments of the knee, providing 85% of the restraining force to anterior tibial displacement at 30 and 90° of knee flexion. The ACL is the most injured ligament of the four located in the knee.

The Segond fracture is a type of avulsion fracture from the lateral tibial plateau of the knee, immediately below the articular surface of the tibia.

Anterior cruciate ligament reconstruction is a surgical tissue graft replacement of the anterior cruciate ligament, located in the knee, to restore its function after an injury. The torn ligament can either be removed from the knee, or preserved before reconstruction through an arthroscopic procedure. ACL repair is also a surgical option. This involves repairing the ACL by re-attaching it, instead of performing a reconstruction. Theoretical advantages of repair include faster recovery and a lack of donor site morbidity, but randomised controlled trials and long-term data regarding re-rupture rates using contemporary surgical techniques are lacking.
The medial collateral ligament (MCL), also called the superficial medial collateral ligament (sMCL) or tibial collateral ligament (TCL), is one of the major ligaments of the knee. It is on the medial (inner) side of the knee joint and occurs in humans and other primates. Its primary function is to resist valgus forces on the knee.

A meniscus is a crescent-shaped fibrocartilaginous anatomical structure that, in contrast to an articular disc, only partly divides a joint cavity. In humans they are present in the knee, wrist, acromioclavicular, sternoclavicular, and temporomandibular joints; in other animals they may be present in other joints.
A meniscus transplant or meniscal transplant is a transplant of the meniscus of the knee, which separates the thigh bone (femur) from the lower leg bone (tibia). The worn or damaged meniscus is removed and is replaced with a new one from a donor. The meniscus to be transplanted is taken from a cadaver, and, as such, is known as an allograft. Meniscal transplantation is technically difficult, as it must be sized accurately for each person, positioned properly and secured to the tibial plateau. As of 2012, only a few surgeons have significant volume of experience in meniscus transplantation worldwide.
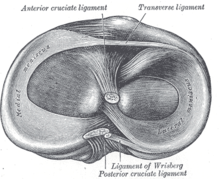
The medial meniscus is a fibrocartilage semicircular band that spans the knee joint medially, located between the medial condyle of the femur and the medial condyle of the tibia. It is also referred to as the internal semilunar fibrocartilage. The medial meniscus has more of a crescent shape while the lateral meniscus is more circular. The anterior aspects of both menisci are connected by the transverse ligament. It is a common site of injury, especially if the knee is twisted.

The lateral meniscus is a fibrocartilaginous band that spans the lateral side of the interior of the knee joint. It is one of two menisci of the knee, the other being the medial meniscus. It is nearly circular and covers a larger portion of the articular surface than the medial. It can occasionally be injured or torn by twisting the knee or applying direct force, as seen in contact sports.
The knee examination, in medicine and physiotherapy, is performed as part of a physical examination, or when a patient presents with knee pain or a history that suggests a pathology of the knee joint.
An anterior cruciate ligament injury occurs when the anterior cruciate ligament (ACL) is either stretched, partially torn, or completely torn. The most common injury is a complete tear. Symptoms include pain, an audible cracking sound during injury, instability of the knee, and joint swelling. Swelling generally appears within a couple of hours. In approximately 50% of cases, other structures of the knee such as surrounding ligaments, cartilage, or meniscus are damaged.

The patellar tendon is the distal portion of the common tendon of the quadriceps femoris, which is continued from the patella to the tibial tuberosity. It is also sometimes called the patellar ligament as it forms a bone to bone connection when the patella is fully ossified.
A tear of a meniscus is a rupturing of one or more of the fibrocartilage strips in the knee called menisci. When doctors and patients refer to "torn cartilage" in the knee, they actually may be referring to an injury to a meniscus at the top of one of the tibiae. Menisci can be torn during innocuous activities such as walking or squatting. They can also be torn by traumatic force encountered in sports or other forms of physical exertion. The traumatic action is most often a twisting movement at the knee while the leg is bent. In older adults, the meniscus can be damaged following prolonged 'wear and tear'. Especially acute injuries can lead to displaced tears which can cause mechanical symptoms such as clicking, catching, or locking during motion of the joint. The joint will be in pain when in use, but when there is no load, the pain goes away.
The transverse or [anterior] meniscomeniscal ligament is a ligament in the knee joint that connects the anterior convex margin of the lateral meniscus to the anterior end of the medial meniscus.
The pivot-shift test is one of the three major tests for assessing anterior cruciate injury or laxity, the other two being the anterior drawer and Lachman test. However, unlike the other two, it tests for instability, an important determinant as to how the knee will function. In fact, it is instability, not simply the injury to the anterior cruciate ligament itself, that places the menisci at future risk, and gives rise to the feeling that the "knee is not secure" or "may give out".

Discoid meniscus is a rare human anatomic variant that usually affects the lateral meniscus of the knee. Usually a person with this anomaly has no complaints; however, it may present as pain, swelling, or a snapping sound heard from the affected knee. Strong suggestive findings on magnetic resonance imaging includes a thickened meniscal body seen on more than two contiguous sagittal slices.
Knee pain is pain in or around the knee.
Posterolateral corner injuries of the knee are injuries to a complex area formed by the interaction of multiple structures. Injuries to the posterolateral corner can be debilitating to the person and require recognition and treatment to avoid long term consequences. Injuries to the PLC often occur in combination with other ligamentous injuries to the knee; most commonly the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). As with any injury, an understanding of the anatomy and functional interactions of the posterolateral corner is important to diagnosing and treating the injury.
Medial knee injuries are the most common type of knee injury. The medial ligament complex of the knee consists of: