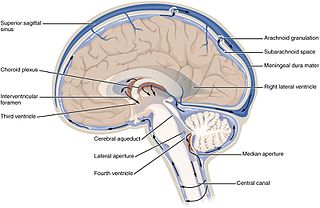
Cerebrospinal fluid (CSF) is a clear, colorless body fluid found within the tissue that surrounds the brain and spinal cord of all vertebrates.
Idiopathic intracranial hypertension (IIH), previously known as pseudotumor cerebri and benign intracranial hypertension, is a condition characterized by increased intracranial pressure without a detectable cause. The main symptoms are headache, vision problems, ringing in the ears, and shoulder pain. Complications may include vision loss.

Papilledema or papilloedema is optic disc swelling that is caused by increased intracranial pressure due to any cause. The swelling is usually bilateral and can occur over a period of hours to weeks. Unilateral presentation is extremely rare.

Hypertensive retinopathy is damage to the retina and retinal circulation due to high blood pressure.

Cerebral edema is excess accumulation of fluid (edema) in the intracellular or extracellular spaces of the brain. This typically causes impaired nerve function, increased pressure within the skull, and can eventually lead to direct compression of brain tissue and blood vessels. Symptoms vary based on the location and extent of edema and generally include headaches, nausea, vomiting, seizures, drowsiness, visual disturbances, dizziness, and in severe cases, death.

Intracranial pressure (ICP) is the pressure exerted by fluids such as cerebrospinal fluid (CSF) inside the skull and on the brain tissue. ICP is measured in millimeters of mercury (mmHg) and at rest, is normally 7–15 mmHg for a supine adult. The body has various mechanisms by which it keeps the ICP stable, with CSF pressures varying by about 1 mmHg in normal adults through shifts in production and absorption of CSF.

Cerebral circulation is the movement of blood through a network of cerebral arteries and veins supplying the brain. The rate of cerebral blood flow in an adult human is typically 750 milliliters per minute, or about 15% of cardiac output. Arteries deliver oxygenated blood, glucose and other nutrients to the brain. Veins carry "used or spent" blood back to the heart, to remove carbon dioxide, lactic acid, and other metabolic products. The neurovascular unit regulates cerebral blood flow so that activated neurons can be supplied with energy in the right amount and at the right time. Because the brain would quickly suffer damage from any stoppage in blood supply, the cerebral circulatory system has safeguards including autoregulation of the blood vessels. The failure of these safeguards may result in a stroke. The volume of blood in circulation is called the cerebral blood flow. Sudden intense accelerations change the gravitational forces perceived by bodies and can severely impair cerebral circulation and normal functions to the point of becoming serious life-threatening conditions.
Cushing reflex is a physiological nervous system response to increased intracranial pressure (ICP) that results in Cushing's triad of increased blood pressure, irregular breathing, and bradycardia. It is usually seen in the terminal stages of acute head injury and may indicate imminent brain herniation. It can also be seen after the intravenous administration of epinephrine and similar drugs. It was first described in detail by American neurosurgeon Harvey Cushing in 1901.

The effects of spaceflight on the human body are complex and largely harmful over both short and long term. Significant adverse effects of long-term weightlessness include muscle atrophy and deterioration of the skeleton. Other significant effects include a slowing of cardiovascular system functions, decreased production of red blood cells, balance disorders, eyesight disorders and changes in the immune system. Additional symptoms include fluid redistribution, loss of body mass, nasal congestion, sleep disturbance, and excess flatulence. Overall, NASA refers to the various deleterious effects of spaceflight on the human body by the acronym RIDGE.

Intraparenchymal hemorrhage (IPH) is one form of intracerebral bleeding in which there is bleeding within brain parenchyma. The other form is intraventricular hemorrhage (IVH).
Cerebral perfusion pressure, or CPP, is the net pressure gradient causing cerebral blood flow to the brain. It must be maintained within narrow limits because too little pressure could cause brain tissue to become ischemic, and too much could raise intracranial pressure (ICP).

Space medicine is an area in aerospace medicine that focuses on the medical care of astronauts and spaceflight participants. The spaceflight environment poses many unique stressors to the human body, including G forces, microgravity, unusual atmospheres such as low pressure or high carbon dioxide, and space radiation. Space medicine applies space physiology, preventive medicine, primary care, emergency medicine, acute care medicine, austere medicine, public health, and toxicology to prevent and treat medical problems in space. This expertise is additionally used to inform vehicle systems design to minimize the risk to human health and performance while meeting mission objectives.

Osmotherapy is the use of osmotically active substances to reduce the volume of intracranial contents. Osmotherapy serves as the primary medical treatment for cerebral edema. The primary purpose of osmotherapy is to improve elasticity and decrease intracranial volume by removing free water, accumulated as a result of cerebral edema, from brain's extracellular and intracellular space into vascular compartment by creating an osmotic gradient between the blood and brain. Normal serum osmolality ranges from 280 to 290 mOsm/kg and serum osmolality to cause water removal from brain without much side effects ranges from 300 to 320 mOsm/kg. Usually, 90 mL of space is created in the intracranial vault by 1.6% reduction in brain water content. Osmotherapy has cerebral dehydrating effects. The main goal of osmotherapy is to decrease intracranial pressure (ICP) by shifting excess fluid from brain. This is accomplished by intravenous administration of osmotic agents which increase serum osmolality in order to shift excess fluid from intracellular or extracellular space of the brain to intravascular compartment. The resulting brain shrinkage effectively reduces intracranial volume and decreases ICP.

Optic disc drusen (ODD) are globules of mucoproteins and mucopolysaccharides that progressively calcify in the optic disc. They are thought to be the remnants of the axonal transport system of degenerated retinal ganglion cells. ODD have also been referred to as congenitally elevated or anomalous discs, pseudopapilledema, pseudoneuritis, buried disc drusen, and disc hyaline bodies.

Weightlessness is the complete or near-complete absence of the sensation of weight, i.e., zero apparent weight. It is also termed zero g-force, or zero-g or, incorrectly, zero gravity.
The monitoring of intracranial pressure (ICP) is used in the treatment of a number of neurological conditions ranging from severe traumatic brain injury to stroke and brain bleeds. This process is called intracranial pressure monitoring. Monitoring is important as persistent increases in ICP is associated with worse prognosis in brain injuries due to decreased oxygen delivery to the injured area and risk of brain herniation.
Increased intracranial pressure (ICP) is one of the major causes of secondary brain ischemia that accompanies a variety of pathological conditions, most notably traumatic brain injury (TBI), strokes, and intracranial hemorrhages. It can cause complications such as vision impairment due to intracranial pressure (VIIP), permanent neurological problems, reversible neurological problems, seizures, stroke, and death. However, aside from a few Level I trauma centers, ICP monitoring is rarely a part of the clinical management of patients with these conditions. The infrequency of ICP can be attributed to the invasive nature of the standard monitoring methods. Additional risks presented to patients can include high costs associated with an ICP sensor's implantation procedure, and the limited access to trained personnel, e.g. a neurosurgeon. Alternative, non-invasive measurement of intracranial pressure, non-invasive methods for estimating ICP have, as a result, been sought.
Space neuroscience or astroneuroscience is the scientific study of the central nervous system (CNS) functions during spaceflight. Living systems can integrate the inputs from the senses to navigate in their environment and to coordinate posture, locomotion, and eye movements. Gravity has a fundamental role in controlling these functions. In weightlessness during spaceflight, integrating the sensory inputs and coordinating motor responses is harder to do because gravity is no longer sensed during free-fall. For example, the otolith organs of the vestibular system no longer signal head tilt relative to gravity when standing. However, they can still sense head translation during body motion. Ambiguities and changes in how the gravitational input is processed can lead to potential errors in perception, which affects spatial orientation and mental representation. Dysfunctions of the vestibular system are common during and immediately after spaceflight, such as space motion sickness in orbit and balance disorders after return to Earth.
Even before the very beginning of human space exploration, serious and reasonable concerns were expressed about exposure of humans to the microgravity of space due to the potential systemic effects on terrestrially-evolved life forms adapted to Earth gravity. Unloading of skeletal muscle, both on Earth via bed-rest experiments and during spaceflight, result in remodeling of muscle. As a result, decrements occur in skeletal muscle strength, fatigue resistance, motor performance, and connective tissue integrity. In addition, there are cardiopulmonary and vascular changes, including a significant decrease in red blood cell mass, that affect skeletal muscle function. This normal adaptive response to the microgravity environment may become a liability resulting in increased risk of an inability or decreased efficiency in crewmember performance of physically demanding tasks during extravehicular activity (EVA) or upon return to Earth.

Cranial venous outflow obstruction, also referred to as impaired cranial venous outflow, impaired cerebral venous outflow, cerebral venous impairment is a vascular disorder that involves the impairment of venous drainage from the cerebral veins of the human brain.









