
Esotropia is a form of strabismus in which one or both eyes turns inward. The condition can be constantly present, or occur intermittently, and can give the affected individual a "cross-eyed" appearance. It is the opposite of exotropia and usually involves more severe axis deviation than esophoria. Esotropia is sometimes erroneously called "lazy eye", which describes the condition of amblyopia; a reduction in vision of one or both eyes that is not the result of any pathology of the eye and cannot be resolved by the use of corrective lenses. Amblyopia can, however, arise as a result of esotropia occurring in childhood: In order to relieve symptoms of diplopia or double vision, the child's brain will ignore or "suppress" the image from the esotropic eye, which when allowed to continue untreated will lead to the development of amblyopia. Treatment options for esotropia include glasses to correct refractive errors, the use of prisms, orthoptic exercises, or eye muscle surgery. The term is from Greek eso meaning "inward" and trope meaning "a turning".

In biology, binocular vision is a type of vision in which an animal has two eyes capable of facing the same direction to perceive a single three-dimensional image of its surroundings. Binocular vision does not typically refer to vision where an animal has eyes on opposite sides of its head and shares no field of view between them, like in some animals.
Orthoptics is a profession allied to the eye care profession. Orthoptists are the experts in diagnosing and treating defects in eye movements and problems with how the eyes work together, called binocular vision. These can be caused by issues with the muscles around the eyes or defects in the nerves enabling the brain to communicate with the eyes. Orthoptists are responsible for the diagnosis and non-surgical management of strabismus (cross-eyed), amblyopia and eye movement disorders. The word orthoptics comes from the Greek words ὀρθός orthos, "straight" and ὀπτικός optikοs, "relating to sight" and much of the practice of orthoptists concerns disorders of binocular vision and defects of eye movement. Orthoptists are trained professionals who specialize in orthoptic treatment, such as eye patches, eye exercises, prisms or glasses. They commonly work with paediatric patients and also adult patients with neurological conditions such as stroke, brain tumours or multiple sclerosis. With specific training, in some countries orthoptists may be involved in monitoring of some forms of eye disease, such as glaucoma, cataract screening and diabetic retinopathy.

Strabismus is a vision disorder in which the eyes do not properly align with each other when looking at an object. The eye that is pointed at an object can alternate. The condition may be present occasionally or constantly. If present during a large part of childhood, it may result in amblyopia, or lazy eyes, and loss of depth perception. If onset is during adulthood, it is more likely to result in double vision.

Amblyopia, also called lazy eye, is a disorder of sight in which the brain fails to fully process input from one eye and over time favors the other eye. It results in decreased vision in an eye that typically appears normal in other aspects. Amblyopia is the most common cause of decreased vision in a single eye among children and younger adults.
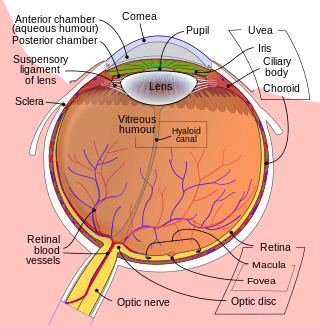
The fovea centralis is a small, central pit composed of closely packed cones in the eye. It is located in the center of the macula lutea of the retina.
The visual field is "that portion of space in which objects are visible at the same moment during steady fixation of the gaze in one direction"; in ophthalmology and neurology the emphasis is mostly on the structure inside the visual field and it is then considered “the field of functional capacity obtained and recorded by means of perimetry”.
Stereopsis is the component of depth perception retrieved by means of binocular disparity through binocular vision. It is not the only contributor to depth perception, but it is a major one. Binocular vision occurs because each eye receives a different image due to their slightly different positions in one's head. These positional differences are referred to as "horizontal disparities" or, more generally, "binocular disparities". Disparities are processed in the visual cortex of the brain to yield depth perception. While binocular disparities are naturally present when viewing a real three-dimensional scene with two eyes, they can also be simulated by artificially presenting two different images separately to each eye using a method called stereoscopy. The perception of depth in such cases is also referred to as "stereoscopic depth".

Eye movement includes the voluntary or involuntary movement of the eyes. Eye movements are used by a number of organisms to fixate, inspect and track visual objects of interests. A special type of eye movement, rapid eye movement, occurs during REM sleep.

A vergence is the simultaneous movement of both eyes in opposite directions to obtain or maintain single binocular vision.

Exotropia is a form of strabismus where the eyes are deviated outward. It is the opposite of esotropia and usually involves more severe axis deviation than exophoria. People with exotropia often experience crossed diplopia. Intermittent exotropia is a fairly common condition. "Sensory exotropia" occurs in the presence of poor vision in one eye. Infantile exotropia is seen during the first year of life, and is less common than "essential exotropia" which usually becomes apparent several years later.

Sixth nerve palsy, or abducens nerve palsy, is a disorder associated with dysfunction of cranial nerve VI, which is responsible for causing contraction of the lateral rectus muscle to abduct the eye. The inability of an eye to turn outward, results in a convergent strabismus or esotropia of which the primary symptom is diplopia in which the two images appear side-by-side. Thus, the diplopia is horizontal and worse in the distance. Diplopia is also increased on looking to the affected side and is partly caused by overaction of the medial rectus on the unaffected side as it tries to provide the extra innervation to the affected lateral rectus. These two muscles are synergists or "yoke muscles" as both attempt to move the eye over to the left or right. The condition is commonly unilateral but can also occur bilaterally.

Congenital fourth nerve palsy is a condition present at birth characterized by a vertical misalignment of the eyes due to a weakness or paralysis of the superior oblique muscle.

The Worth Four Light Test, also known as the Worth's four dot test or W4LT, is a clinical test mainly used for assessing a patient's degree of binocular vision and binocular single vision. Binocular vision involves an image being projected by each eye simultaneously into an area in space and being fused into a single image. The Worth Four Light Test is also used in detection of suppression of either the right or left eye. Suppression occurs during binocular vision when the brain does not process the information received from either of the eyes. This is a common adaptation to strabismus, amblyopia and aniseikonia.
Suppression of an eye is a subconscious adaptation by a person's brain to eliminate the symptoms of disorders of binocular vision such as strabismus, convergence insufficiency and aniseikonia. The brain can eliminate double vision by ignoring all or part of the image of one of the eyes. The area of a person's visual field that is suppressed is called the suppression scotoma. Suppression can lead to amblyopia.
Cyclotropia is a form of strabismus in which, compared to the correct positioning of the eyes, there is a torsion of one eye about the eye's visual axis. Consequently, the visual fields of the two eyes appear tilted relative to each other. The corresponding latent condition – a condition in which torsion occurs only in the absence of appropriate visual stimuli – is called cyclophoria.

Stereopsis recovery, also recovery from stereoblindness, is the phenomenon of a stereoblind person gaining partial or full ability of stereo vision (stereopsis).
In ophthalmology, horror fusionis is a condition in which the eyes have an unsteady deviation, with the extraocular muscles performing spasm-like movements that continuously shift the eyes away from the position in which they would be directed to the same point in space, giving rise to diplopia. Even when the double vision images are made to nearly overlap using optical means such as prisms, the irregular movements prevent binocular fusion. The name horror fusionis arises from the notion that the brain is, or at least appears to be, actively preventing binocular fusion.
The management of strabismus may include the use of drugs or surgery to correct the strabismus. Agents used include paralytic agents such as botox used on extraocular muscles, topical autonomic nervous system agents to alter the refractive index in the eyes, and agents that act in the central nervous system to correct amblyopia.
Retinal birefringence scanning (RBS) is a method for detecting the central fixation of the eye. The method can be used in pediatric ophthalmology for screening purposes. By simultaneously measuring the central fixation of both eyes, small- and large-angle strabismus can be detected. The method is not invasive and requires little cooperation by the patient, so it can be used for detecting strabismus in young children. The method provides a reliable detection of strabismus and has also been used for detecting certain kinds of amblyopia. RBS uses the human eye's birefringent properties to identify the position of the fovea and the direction of gaze, and thereby to measure any binocular misalignment.
