
A coma is a deep state of prolonged unconsciousness in which a person cannot be awakened, fails to respond normally to painful stimuli, light, or sound, lacks a normal wake-sleep cycle and does not initiate voluntary actions. The person may experience respiratory and circulatory problems due to the body's inability to maintain normal bodily functions. People in a coma often require extensive medical care to maintain their health and prevent complications such as pneumonia or blood clots. Coma patients exhibit a complete absence of wakefulness and are unable to consciously feel, speak or move. Comas can be derived by natural causes, or can be medically induced.

A cerebral arteriovenous malformation is an abnormal connection between the arteries and veins in the brain—specifically, an arteriovenous malformation in the cerebrum.

Death is the irreversible cessation of all biological functions that sustain a living organism. The remains of a former organism normally begin to decompose shortly after death. Death eventually and inevitably occurs in all organisms. Some organisms, such as Turritopsis dohrnii, are biologically immortal, however they can still die from means other than aging. Death is generally applied to whole organisms; the equivalent for individual components of an organism, such as cells or tissues, is necrosis. Something that is not considered an organism, such as a virus, can be physically destroyed but is not said to die, as a virus is not considered alive in the first place.

Locked-in syndrome (LIS), also known as pseudocoma, is a condition in which a patient is aware but cannot move or communicate verbally due to complete paralysis of nearly all voluntary muscles in the body except for vertical eye movements and blinking. The individual is conscious and sufficiently intact cognitively to be able to communicate with eye movements. Electroencephalography results are normal in locked-in syndrome. Total locked-in syndrome, or completely locked-in state (CLIS), is a version of locked-in syndrome wherein the eyes are paralyzed as well. Fred Plum and Jerome B. Posner coined the term for this disorder in 1966.

Anencephaly is the absence of a major portion of the brain, skull, and scalp that occurs during embryonic development. It is a cephalic disorder that results from a neural tube defect that occurs when the rostral (head) end of the neural tube fails to close, usually between the 23rd and 26th day following conception. Strictly speaking, the Greek term translates as "without a brain", but it is accepted that children born with this disorder usually only lack a telencephalon, the largest part of the brain consisting mainly of the cerebral hemispheres, including the neocortex, which is responsible for cognition. The remaining structure is usually covered only by a thin layer of membrane—skin, bone, meninges, etc., are all lacking. With very few exceptions, infants with this disorder do not survive longer than a few hours or days after birth.
A vegetative state (VS) or post-coma unresponsiveness (PCU) is a disorder of consciousness in which patients with severe brain damage are in a state of partial arousal rather than true awareness. After four weeks in a vegetative state, the patient is classified as being in a persistent vegetative state (PVS). This diagnosis is classified as a permanent vegetative state some months after a non-traumatic brain injury or one year after a traumatic injury. The term unresponsive wakefulness syndrome may be alternatively used, as "vegetative state" has some negative connotations among the public.
Prior to the introduction of brain death into law in the mid to late 1970s, all organ transplants from cadaveric donors came from non-heart-beating donors (NHBDs).

Intracranial hemorrhage (ICH), also known as intracranial bleed, is bleeding within the skull. Subtypes are intracerebral bleeds, subarachnoid bleeds, epidural bleeds, and subdural bleeds.
A flatline is an electrical time sequence measurement that shows no activity and therefore, when represented, shows a flat line instead of a moving one. It almost always refers to either a flatlined electrocardiogram, where the heart shows no electrical activity (asystole), or to a flat electroencephalogram, in which the brain shows no electrical activity. Both of these specific cases are involved in various definitions of death.
Central neurogenic hyperventilation (CNH) is an abnormal pattern of breathing characterized by deep and rapid breaths at a rate of at least 25 breaths per minute. Increasing irregularity of this respiratory rate generally is a sign that the patient will enter into coma. CNH is unrelated to other forms of hyperventilation, like Kussmaul's respirations. CNH is the human body's response to reduced carbon dioxide levels in the blood. This reduction in carbon dioxide is caused by contraction of cranial arteries from damage caused by lesions in the brain stem. However, the mechanism by which CNH arises as a result from these lesions is still very poorly understood. Current research has yet to provide an effective means of treatment for the rare number of patients who are diagnosed with this condition.

A watershed stroke is defined as a brain ischemia that is localized to the vulnerable border zones between the tissues supplied by the anterior, posterior and middle cerebral arteries. The actual blood stream blockage/restriction site can be located far away from the infarcts. Watershed locations are those border-zone regions in the brain supplied by the major cerebral arteries where blood supply is decreased. Watershed strokes are a concern because they comprise approximately 10% of all ischemic stroke cases. The watershed zones themselves are particularly susceptible to infarction from global ischemia as the distal nature of the vasculature predisposes these areas to be most sensitive to profound hypoperfusion.

Vertebral artery dissection (VAD) is a flap-like tear of the inner lining of the vertebral artery, which is located in the neck and supplies blood to the brain. After the tear, blood enters the arterial wall and forms a blood clot, thickening the artery wall and often impeding blood flow. The symptoms of vertebral artery dissection include head and neck pain and intermittent or permanent stroke symptoms such as difficulty speaking, impaired coordination, and visual loss. It is usually diagnosed with a contrast-enhanced CT or MRI scan.
Certain fundamental Jewish law questions arise in issues of organ donation. Donation of an organ from a living person to save another's life, where the donor's health will not appreciably suffer, is permitted and encouraged in Jewish law. Donation of an organ from a dead person is equally permitted for the same purpose: to save a life. This simple statement of the issue belies, however, the complexity of defining death in Jewish law. Thus, although there are side issues regarding mutilation of the body etc., the primary issue that prevents organ donation from the dead amongst Jews, in many cases, is the definition of death, simply because to take a life-sustaining organ from a person who was still alive would be murder.

The Lazarus sign or Lazarus reflex is a reflex movement in brain-dead or brainstem failure patients, which causes them to briefly raise their arms and drop them crossed on their chests. The phenomenon is named after the Biblical figure Lazarus of Bethany, whom Jesus raised from the dead according to the Gospel of John.
A beating heart cadaver is a body that is pronounced dead in all medical and legal definitions, connected to a medical ventilator, and retains cardio-pulmonary functions. This keeps the organs of the body, including the heart, functioning and alive. As a result, the period of time in which the organs may be used for transplantation is extended. The heart contains pacemaker cells that will cause it to continue beating even when a patient is brain-dead. Other organs in the body do not have this capability and need the brain to be functioning to send signals to the organs to carry out their functions. A beating heart cadaver requires a ventilator to provide oxygen to its blood, but the heart will continue to beat on its own even in the absence of brain activity. This allows organs to be preserved for a longer period of time in the case of a transplant or donation. A small number of cases in recent years indicate that it can also be implemented for a brain-dead pregnant woman to reach the full term of her pregnancy. There is an advantage to beating heart cadaver organ donation because doctors are able to see the vitals of the organs and tell if they are stable and functioning before transplanting to an ailing patient. This is not possible in a donation from someone pronounced dead.
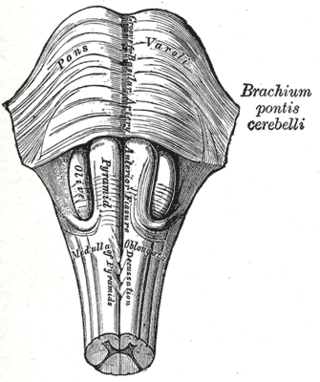
Brainstem death is a clinical syndrome defined by the absence of reflexes with pathways through the brainstem – the "stalk" of the brain, which connects the spinal cord to the mid-brain, cerebellum and cerebral hemispheres – in a deeply comatose, ventilator-dependent patient. Identification of this state carries a very grave prognosis for survival; cessation of heartbeat often occurs within a few days, although it may continue for weeks if intensive support is maintained.
Bickerstaff brainstem encephalitis is a rare inflammatory disorder of the central nervous system, first described by Edwin Bickerstaff in 1951. It may also affect the peripheral nervous system, and has features in common with both Miller Fisher syndrome and Guillain–Barré syndrome.
Disorders of consciousness are medical conditions that inhibit consciousness. Some define disorders of consciousness as any change from complete self-awareness to inhibited or absent self-awareness and arousal. This category generally includes minimally conscious state and persistent vegetative state, but sometimes also includes the less severe locked-in syndrome and more severe but rare chronic coma. Differential diagnosis of these disorders is an active area of biomedical research. Finally, brain death results in an irreversible disruption of consciousness. While other conditions may cause a moderate deterioration or transient interruption of consciousness, they are not included in this category.
Legal death is the recognition under the law of a particular jurisdiction that a person is no longer alive. In most cases, a doctor's declaration of death or the identification of a corpse is a legal requirement for such recognition. A person who has been missing for a sufficiently long period of time may be presumed or declared legally dead, usually by a court. When a death has been registered in a civil registry, a death certificate may be issued. Such death certificate may be required in a number of legal situations, such as applying for probate, claiming some benefits, or making an insurance claim.
The stages of death of a human being have medical, biochemical and legal aspects. The term taphonomy from palaeontology applies to the fate of all kinds of remains of organisms. Forensic taphonomy is concerned with remains of the human body.
