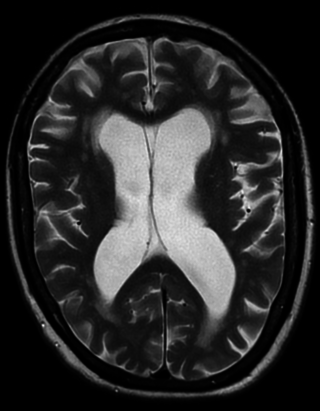
Vascular dementia is dementia caused by a series of strokes. Restricted blood flow due to strokes reduces oxygen and glucose delivery to the brain, causing cell injury and neurological deficits in the affected region. Subtypes of vascular dementia include subcortical vascular dementia, multi-infarct dementia, stroke-related dementia, and mixed dementia.

Lifestyle diseases can be defined as the diseases linked to the manner in which a person lives their life. These diseases are non-communicable, and can be caused by lack of physical activity, unhealthy eating, alcohol, substance use disorders and smoking tobacco, which can lead to heart disease, stroke, obesity, type II diabetes and lung cancer. The diseases that appear to increase in frequency as countries become more industrialized and people live longer include Alzheimer's disease, arthritis, atherosclerosis, asthma, cancer, chronic liver disease or cirrhosis, chronic obstructive pulmonary disease, colitis, irritable bowel syndrome, type 2 diabetes, heart disease, hypertension, metabolic syndrome, chronic kidney failure, osteoporosis, PCOD, stroke, depression, obesity and vascular dementia.

Preventive healthcare, or prophylaxis, is the application of healthcare measures to prevent diseases. Disease and disability are affected by environmental factors, genetic predisposition, disease agents, and lifestyle choices, and are dynamic processes that begin before individuals realize they are affected. Disease prevention relies on anticipatory actions that can be categorized as primal, primary, secondary, and tertiary prevention.
A chronic condition is a health condition or disease that is persistent or otherwise long-lasting in its effects or a disease that comes with time. The term chronic is often applied when the course of the disease lasts for more than three months. Common chronic diseases include diabetes, functional gastrointestinal disorder, eczema, arthritis, asthma, chronic obstructive pulmonary disease, autoimmune diseases, genetic disorders and some viral diseases such as hepatitis C and acquired immunodeficiency syndrome. An illness which is lifelong because it ends in death is a terminal illness. It is possible and not unexpected for an illness to change in definition from terminal to chronic. Diabetes and HIV for example were once terminal yet are now considered chronic due to the availability of insulin for diabetics and daily drug treatment for individuals with HIV which allow these individuals to live while managing symptoms.
Diseases of poverty are diseases that are more prevalent in low-income populations. They include infectious diseases, as well as diseases related to malnutrition and poor health behaviour. Poverty is one of the major social determinants of health. The World Health Report (2002) states that diseases of poverty account for 45% of the disease burden in the countries with high poverty rate which are preventable or treatable with existing interventions. Diseases of poverty are often co-morbid and ubiquitous with malnutrition. Poverty increases the chances of having these diseases as the deprivation of shelter, safe drinking water, nutritious food, sanitation, and access to health services contributes towards poor health behaviour. At the same time, these diseases act as a barrier for economic growth to affected people and families caring for them which in turn results into increased poverty in the community. These diseases produced in part by poverty are in contrast to diseases of affluence, which are diseases thought to be a result of increasing wealth in a society.

A non-communicable disease (NCD) is a disease that is not transmissible directly from one person to another. NCDs include Parkinson's disease, autoimmune diseases, strokes, heart diseases, cancers, diabetes, chronic kidney disease, osteoarthritis, osteoporosis, Alzheimer's disease, cataracts, and others. NCDs may be chronic or acute. Most are non-infectious, although there are some non-communicable infectious diseases, such as parasitic diseases in which the parasite's life cycle does not include direct host-to-host transmission.

An aging-associated disease is a disease that is most often seen with increasing frequency with increasing senescence. They are essentially complications of senescence, distinguished from the aging process itself because all adult animals age but not all adult animals experience all age-associated diseases. The term does not refer to age-specific diseases, such as the childhood diseases chicken pox and measles, only diseases of the elderly. They are also not accelerated aging diseases, all of which are genetic disorders.

Health may refer to "a state of complete physical, mental and social well-being and not merely the absence of disease and infirmity.", according to the World Health Organization (WHO). 78.7 was the average life expectancy for individuals at birth in 2017. The highest cause of death for United States citizens is heart disease. Sexually transmitted infections impact the health of approximately 19 million yearly. The two most commonly reported infections include chlamydia and gonorrhea. The United States is currently challenged by the COVID-19 pandemic, and is 19th in the world in COVID-19 vaccination rates. All 50 states in the U.S. require immunizations for children in order to enroll in public school, but various exemptions are available by state. Immunizations are often compulsory for military enlistment in the United States.
Australia is a high income country, and this is reflected in the good status of health of the population overall. In 2011, Australia ranked 2nd on the United Nations Development Programme's Human Development Index, indicating the level of development of a country. Despite the overall good status of health, the disparities occurring in the Australian healthcare system are a problem. The poor and those living in remote areas as well as indigenous people are, in general, less healthy than others in the population, and programs have been implemented to decrease this gap. These include increased outreach to the indigenous communities and government subsidies to provide services for people in remote or rural areas.
Social epidemiology focuses on the patterns in morbidity and mortality rates that emerge as a result of social characteristics. While an individual's lifestyle choices or family history may place him or her at an increased risk for developing certain illnesses, there are social inequalities in health that cannot be explained by individual factors. Variations in health outcomes in the United States are attributed to several social characteristics, such as gender, race, socioeconomic status, the environment, and educational attainment. Inequalities in any or all of these social categories can contribute to health disparities, with some groups placed at an increased risk for acquiring chronic diseases than others.
Chronic, non-communicable diseases account for an estimated 80% of total deaths and 70% of disability-adjusted life years (DALYs) lost in China. Cardiovascular diseases, chronic respiratory disease, and cancer are the leading causes of both death and of the burden of disease, and exposure to risk factors is high: more than 300 million men smoke cigarettes and 160 million adults are hypertensive, most of whom are not being treated. An obesity epidemic is imminent, with more than 20% of children aged 7–17 years in big cities now overweight or obese. Rates of death from chronic disease in middle-aged people are higher in China than in some high-income countries.

The major causes of deaths in Finland are cardiovascular diseases, malignant tumors, dementia and Alzheimer's disease, respiratory diseases, alcohol related diseases and accidental poisoning by alcohol. In 2010, the leading causes of death among men aged 15 to 64 were alcohol related deaths, ischaemic heart disease, accident, suicides, lung cancer and cerebrovascular diseases. Among women the leading causes were breast cancer, alcohol related deaths, accidents, suicides, ischaemic heart disease and lung cancer.

Brunei's healthcare system is managed by the Brunei Ministry of Health and funded by the General Treasury. It consists of around 15 health centers, ten clinics and 22 maternal facilities, considered to be of reasonable standard. There are also two private hospitals. Cardiovascular disease, cancer, and diabetes are the leading cause of death in the country, with life expectancy around 75 years, a vast improvement from 1961. Brunei's human development index (HCI) improved from 0.81 in 2002 to 0.83 in 2021, expanding at an average annual rate of 0.14%. According to the UN's Human Development Report 2020, the HCI for girls in the country is greater than for boys, though aren't enough statistics in Brunei to break down HCI by socioeconomic classes. Brunei is the second country in Southeast Asia after Singapore to be rated 47th out of 189 nations on the UN HDI 2019 and has maintained its position in the Very High Human Development category. Being a culturally taboo subject, the rate of suicide has not been investigated.
This article provides a global overview of the current trends and distribution of metabolic syndrome. Metabolic syndrome refers to a cluster of related risk factors for cardiovascular disease that includes abdominal obesity, diabetes, hypertension, and elevated cholesterol.

Globally, an estimated 537 million adults are living with diabetes, according to 2019 data from the International Diabetes Federation. Diabetes was the 9th-leading cause of mortality globally in 2020, attributing to over 2 million deaths annually due to diabetes directly, and to kidney disease due to diabetes. The primary causes of type 2 diabetes is diet and physical activity, which can contribute to increased BMI, poor nutrition, hypertension, alcohol use and smoking, while genetics is also a factor. Diabetes prevalence is increasing rapidly; previous 2019 estimates put the number at 463 million people living with diabetes, with the distributions being equal between both sexes icidence peaking around age 55 years old. The number is projected to 643 million by 2030, or 7079 individuals per 100,000, with all regions around the world continue to rise. Type 2 diabetes makes up about 85-90% of all cases. Increases in the overall diabetes prevalence rates largely reflect an increase in risk factors for type 2, notably greater longevity and being overweight or obese. The prevalence of African Americans with diabetes is estimated to triple by 2050, while the prevalence of whites is estimated to double. The overall prevalence increases with age, with the largest increase in people over 65 years of age. The prevalence of diabetes in America is estimated to increase to 48.3 million by 2050.
Montenegro is a country with an area of 13,812 square kilometres and a population of 620,029, according to the 2011 census. The country is bordered by Croatia, the Adriatic Sea, Bosnia, Herzegovina, Serbia, Kosovo and Albania. The most common health issues faced are non-communicable diseases accounting for 95% of all deaths. This is followed by 4% of mortality due to injury, and 1% due to communicable, maternal, perinatal and nutritional conditions. Other health areas of interest are alcohol consumption, which is the most prevalent disease of addiction within Montenegro and smoking. Montenegro has one of the highest tobacco usage rates across Europe. Life expectancy for men is 74 years, and life expectancy for women is 79.

Dementia and Alzheimer's disease in Australia is a major health issue. Alzheimer's disease is the most common type of dementia in Australia. Dementia is an ever-increasing challenge as the population ages and life expectancy increases. As a consequence, there is an expected increase in the number of people with dementia, posing countless challenges to carers and the health and aged care systems. In 2018, an estimated 376,000 people had dementia; this number is expected to increase to 550,000 by 2030 and triple to 900,000 by 2050. The dementia death rate is increasing, resulting in the shift from fourth to second leading cause of death from 2006 to 2015. It is expected to become the leading cause of death over the next number of years. In 2011, it was the fourth leading cause of disease burden and third leading cause of disability burden. This is expected to remain the same until at least 2020.
Native Americans are affected by noncommunicable illnesses related to social changes and contemporary eating habits. Increasing rates of obesity, poor nutrition, sedentary lifestyle, and social isolation affect many Americans. While subject to the same illnesses, Native Americans have higher morbidity and mortality to diabetes and cardiovascular disease as well as certain forms of cancer. Social and historical factors tend to promote unhealthy behaviors including suicide and alcohol dependence. Reduced access to health care in Native American communities means that these diseases as well as infections affect more people for longer periods of time.
Alzheimer's disease (AD) in African Americans is becoming a rising topic of interest in AD care, support, and scientific research, as African Americans are disproportionately affected by AD. Recent research on AD has shown that there are clear disparities in the disease among racial groups, with higher prevalence and incidence in African Americans than the overall average. Pathologies for Alzheimer’s also seem to manifest differently in African Americans, including with neuroinflammation markers, cognitive decline, and biomarkers. Although there are genetic risk factors for Alzheimer’s, these account for few cases in all racial groups.