
Migraine is a genetically influenced complex neurological disorder characterized by episodes of moderate-to-severe headache, most often unilateral and generally associated with nausea and light and sound sensitivity. Other characterizing symptoms may include nausea, vomiting, cognitive dysfunction, allodynia, and dizziness. Exacerbation of headache symptoms during physical activity is another distinguishing feature. Up to one-third of migraine sufferers experience aura, a premonitory period of sensory disturbance widely accepted to be caused by cortical spreading depression at the onset of a migraine attack. Although primarily considered to be a headache disorder, migraine is highly heterogenous in its clinical presentation and is better thought of as a spectrum disease rather than a distinct clinical entity. Disease burden can range from episodic discrete attacks, consisting of as little as several lifetime attacks, to chronic disease.

Headache, also known as cephalalgia, is the symptom of pain in the face, head, or neck. It can occur as a migraine, tension-type headache, or cluster headache. There is an increased risk of depression in those with severe headaches.
Cluster headache is a neurological disorder characterized by recurrent severe headaches on one side of the head, typically around the eye(s). There is often accompanying eye watering, nasal congestion, or swelling around the eye on the affected side. These symptoms typically last 15 minutes to 3 hours. Attacks often occur in clusters which typically last for weeks or months and occasionally more than a year.
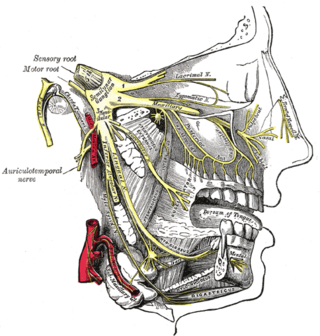
Trigeminal neuralgia, also called Fothergill disease, tic douloureux, trifacial neuralgia, or suicide disease, is a long-term pain disorder that affects the trigeminal nerve, the nerve responsible for sensation in the face and motor functions such as biting and chewing. It is a form of neuropathic pain. There are two main types: typical and atypical trigeminal neuralgia. The typical form results in episodes of severe, sudden, shock-like pain in one side of the face that lasts for seconds to a few minutes. Groups of these episodes can occur over a few hours. The atypical form results in a constant burning pain that is less severe. Episodes may be triggered by any touch to the face. Both forms may occur in the same person. It is regarded as one of the most painful disorders known to medicine, and often results in depression and suicide.
Triptans are a family of tryptamine-based drugs used as abortive medication in the treatment of migraines and cluster headaches. This drug class was first commercially introduced in the 1990s. While effective at treating individual headaches, they do not provide preventive treatment and are not considered a cure. They are not effective for the treatment of tension–type headache, except in persons who also experience migraines. Triptans do not relieve other kinds of pain.
Chronic paroxysmal hemicrania (CPH) is a severe debilitating unilateral headache usually affecting the area around the eye. It normally consists of multiple severe, yet short, headache attacks affecting only one side of the cranium. Retrospective surveys indicated that paroxysmal hemicrania was more common in women. However, subsequent prospective research showed an equal prevalence between females and males, with a ratio close to 1:1. Unlike in migraine, it has no neurological symptoms associated with it. CPH headaches are treated through the use of non-steroidal anti-inflammatory drugs, with indomethacin found to be especially effective in eliminating symptoms.
The Nociceptive trigeminal inhibition tension suppression system, is a type of occlusal splint that is claimed to prevent headache and migraine by reducing sleep bruxism. Sleep bruxism is purported to lead to a hyperactivity of the trigeminal nerve, often triggering typical migraine events. The hyperactivity of trigeminal neurons during trigemino-nociceptive stimulation is a proposed cause of migraine and is correlated with imaging of migraine sufferers. The objective of the NTI-TSS is to relax the muscles involved in clenching and bruxing, thus supposedly diminishing the chances for migraines and tension headaches to develop through the reduction in nociceptive stimulation normally caused by parafunctional activity. It is sometimes used for temporomandibular joint dysfunction (TMD).
Hemicrania continua (HC) is a persistent unilateral headache that responds to indomethacin. It is usually unremitting, but rare cases of remission have been documented. Hemicrania continua is considered a primary headache disorder, meaning that another condition does not cause it.

Tolosa–Hunt syndrome is a rare disorder characterized by severe and unilateral headaches with orbital pain, along with weakness and paralysis (ophthalmoplegia) of certain eye muscles.
Geniculate ganglionitis or geniculate neuralgia (GN), also called nervus intermedius neuralgia, Ramsay Hunt syndrome, or Hunt's neuralgia, is a rare disorder characterized by severe paroxysmal neuralgic pain deep in the ear, that may spread to the ear canal, outer ear, mastoid or eye regions. GN may also occur in combination with trigeminal or glossopharyngeal neuralgia.

Orthostatic headache is a medical condition in which a person develops a headache while vertical and the headache is relieved when horizontal. Previously it was often misdiagnosed as different primary headache disorders such as migraine or tension headaches. Increasing awareness of the symptom and its causes has prevented delayed or missed diagnosis.
New daily persistent headache (NDPH) is a primary headache syndrome which can mimic chronic migraine and chronic tension-type headache. The headache is daily and unremitting from very soon after onset, usually in a person who does not have a history of a primary headache disorder. The pain can be intermittent, but lasts more than 3 months. Headache onset is abrupt and people often remember the date, circumstance and, occasionally, the time of headache onset. One retrospective study stated that over 80% of patients could state the exact date their headache began.
The International Classification of Headache Disorders (ICHD) is a detailed hierarchical classification of all headache-related disorders published by the International Headache Society. It is considered the official classification of headaches by the World Health Organization, and, in 1992, was incorporated into the 10th edition of their International Classification of Diseases (ICD-10). Each class of headache contains explicit diagnostic criteria—meaning that the criteria include quantities rather than vague terms like several or usually—that are based on clinical and laboratory observations.

A cerebrospinal fluid leak is a medical condition where the cerebrospinal fluid (CSF) that surrounds the brain and spinal cord leaks out of one or more holes or tears in the dura mater. A CSF leak is classed as either spontaneous (primary), having no known cause, or nonspontaneous (secondary) where it is attributed to an underlying condition. Causes of a primary CSF leak are those of trauma including from an accident or intentional injury, or arising from a medical intervention known as iatrogenic. A basilar skull fracture as a cause can give the sign of CSF leakage from the ear nose or mouth. A lumbar puncture can give the symptom of a post-dural-puncture headache.
The classification of all headaches, including migraines, is organized by the International Headache Society, and published in the International Classification of Headache Disorders (ICHD). The current version, the ICHD-3 beta, was published in 2013.

Red ear syndrome (RES) is a rare disorder of unknown etiology which was originally described in 1994. The defining symptom of red ear syndrome is redness of one or both external ears, accompanied by a burning sensation. A variety of treatments have been tried with limited success.
Trigeminal autonomic cephalalgia (TAC) refers to a group of primary headaches that occurs with pain on one side of the head in the trigeminal nerve area and symptoms in autonomic systems on the same side, such as eye watering and redness or drooping eyelids.
Neck-tongue syndrome (NTS), which was first recorded in 1980, is a rare disorder characterized by neck pain with or without tingling and numbness of the tongue on the same side as the neck pain. Sharp lateral movement of the head triggers the pain, usually lasting from a few seconds to a few minutes. Headaches may occur with the onset of NTS. The typical age of onset is around adolescence and may occur as early as 8–15 years old. However, it is worth noting that clinical onset can occur earlier or later and NTS onset related to trauma can occur at any age, beginning after the incident.
Craniocervical instability (CCI) is a medical condition characterized by excessive movement of the vertebra at the atlanto-occipital joint and the atlanto-axial joint located between the skull and the top two vertebra, known as C1 and C2. The condition can cause neural injury and compression of nearby structures, including the brain stem, spinal cord, vagus nerve, and vertebral artery, resulting in a constellation of symptoms.

Recurrent painful ophthalmoplegic neuropathy (RPON), previously known as ophthalmoplegic migraine (OM), is a rare neurological disorder that is characterized by repeated headache attacks and reversible ipsilateral paresis of one or more ocular cranial nerves (CN). Oculomotor nerve (CNIII) is by far the most common cranial nerve involves in RPON, while abducens nerve (CNVI) and trochlear nerve (CNIV) involvements are also reported. Globally, RPON was estimated to have an annual incidence rate of 0.7 per million as of 1990, no further epidemiological studies have been conducted. It occurs more often in children and females.