Major depressive disorder (MDD), also known as clinical depression, is a mental disorder characterized by at least two weeks of pervasive low mood, low self-esteem, and loss of interest or pleasure in normally enjoyable activities. Introduced by a group of US clinicians in the mid-1970s, the term was adopted by the American Psychiatric Association for this symptom cluster under mood disorders in the 1980 version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III), and has become widely used since.
Suicide is the second leading cause of death for people in the United States from the ages of 9 to 56.
Adjustment disorder is a maladaptive response to a psychosocial stressor. It is classified as a mental disorder. The maladaptive response usually involves otherwise normal emotional and behavioral reactions that manifest more intensely than usual, causing marked distress, preoccupation with the stressor and its consequences, and functional impairment.
Child psychopathology refers to the scientific study of mental disorders in children and adolescents. Oppositional defiant disorder, attention-deficit hyperactivity disorder, and autism spectrum disorder are examples of psychopathology that are typically first diagnosed during childhood. Mental health providers who work with children and adolescents are informed by research in developmental psychology, clinical child psychology, and family systems. Lists of child and adult mental disorders can be found in the International Statistical Classification of Diseases and Related Health Problems, 10th Edition (ICD-10), published by the World Health Organization (WHO) and in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), published by the American Psychiatric Association (APA). In addition, the Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood is used in assessing mental health and developmental disorders in children up to age five.
Suicide intervention is a direct effort to prevent a person or persons from attempting to take their own life or lives intentionally.

Suicidal ideation, or suicidal thoughts, is the thought process of having ideas, or ruminations about the possibility of completing suicide. It is not a diagnosis but is a symptom of some mental disorders, use of certain psychoactive drugs, and can also occur in response to adverse life events without the presence of a mental disorder.
A major depressive episode (MDE) is a period characterized by symptoms of major depressive disorder. Those affected primarily exhibit a depressive mood for at least two weeks or more, and a loss of interest or pleasure in everyday activities. Other symptoms can include feelings of emptiness, hopelessness, anxiety, worthlessness, guilt, irritability, changes in appetite, difficulties in concentration, difficulties remembering details, making decisions, and thoughts of suicide. Insomnia or hypersomnia and aches, pains, or digestive problems that are resistant to treatment may also be present.
Suicide risk assessment is a process of estimating the likelihood for a person to attempt or die by suicide. The goal of a thorough risk assessment is to learn about the circumstances of an individual person with regard to suicide, including warning signs, risk factors, and protective factors. Risk for suicide is re-evaluated throughout the course of care to assess the patient's response to personal situational changes and clinical interventions. Accurate and defensible risk assessment requires a clinician to integrate a clinical judgment with the latest evidence-based practice, although accurate prediction of low base rate events, such as suicide, is inherently difficult and prone to false positives.
A suicide crisis, suicidal crisis or potential suicide is a situation in which a person is attempting to kill themselves or is seriously contemplating or planning to do so. It is considered by public safety authorities, medical practice, and emergency services to be a medical emergency, requiring immediate suicide intervention and emergency medical treatment. Suicidal presentations occur when an individual faces an emotional, physical, or social problem they feel they cannot overcome and considers suicide to be a solution. Clinicians usually attempt to re-frame suicidal crises, point out that suicide is not a solution and help the individual identify and solve or tolerate the problems.
Youth suicide is when a young person, generally categorized as someone below the legal age of majority, deliberately ends their own life. Rates of youth suicide and attempted youth suicide in Western societies and other countries are high. Youth suicide attempts are more common among girls, but adolescent males are the ones who usually carry out suicide. Suicide rates in youths have nearly tripled between the 1960s and 1980s. For example, in Australia suicide is second only to motor vehicle accidents as its leading cause of death for people aged 15 to 25.

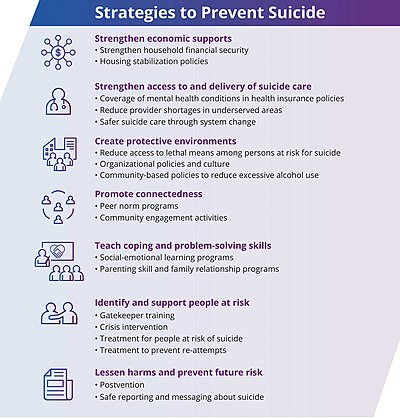
Suicide is the act of intentionally causing one's own death. Mental disorders, physical disorders, and substance abuse are risk factors. Some suicides are impulsive acts due to stress, relationship problems, or harassment and bullying. Those who have previously attempted suicide are at a higher risk for future attempts. Effective suicide prevention efforts include limiting access to methods of suicide such as firearms, drugs, and poisons; treating mental disorders and substance abuse; careful media reporting about suicide; improving economic conditions; and dialectical behaviour therapy (DBT). Although crisis hotlines are common resources, their effectiveness has not been well studied.

Major depressive disorder, often simply referred to as depression, is a mental disorder characterized by prolonged unhappiness or irritability. It is accompanied by a constellation of somatic and cognitive signs and symptoms such as fatigue, apathy, sleep problems, loss of appetite, loss of engagement, low self-regard/worthlessness, difficulty concentrating or indecisiveness, or recurrent thoughts of death or suicide.

Depression, one of the most commonly diagnosed psychiatric disorders, is being diagnosed in increasing numbers in various segments of the population worldwide. Depression in the United States alone affects 17.6 million Americans each year or 1 in 6 people. Depressed patients are at increased risk of type 2 diabetes, cardiovascular disease and suicide. Within the next twenty years depression is expected to become the second leading cause of disability worldwide and the leading cause in high-income nations, including the United States. In approximately 75% of suicides, the individuals had seen a physician within the prior year before their death, 45–66% within the prior month. About a third of those who died by suicide had contact with mental health services in the prior year, a fifth within the preceding month.

Igor Galynker is an American psychiatrist, clinician and researcher. His research interests include bipolar disorder, suicide prevention, and the role of family dynamics in psychiatric illness. He has published on these topics both in professional journals and in the lay press. His recent research has been devoted to describing Suicide Crisis Syndrome (SCS), an acute suicidal cognitive-affective state predictive of imminent suicidal behavior.
In 2014, the WHO ranked Nepal as the 7th in the global suicide rate. The estimated annual suicides in Nepal are 6,840 or 24.9 suicides per 100,000 people. Data on suicide in Nepal are primarily based on police reports and therefore rely on mortality statistics. However, the burden of suicide in communities is likely to be higher, particularly among women, migrant workers, and populations affected by disasters.
In colleges and universities in the United States, suicide is one of the most common causes of death among students. Each year, approximately 24,000 college students attempt suicide while 1,100 students succeed in their attempt, making suicide the second-leading cause of death among U.S. college students. Roughly 12% of college students report the occurrence of suicide ideation during their first four years in college, with 2.6% percent reporting persistent suicide ideation. 65% of college students reported that they knew someone who has either attempted or died by suicide, showing that the majority of students on college campuses are exposed to suicide or suicidal attempts.
Prevention of mental disorders are measures that try to decrease the chances of a mental disorder occurring. A 2004 WHO report stated that "prevention of these disorders is obviously one of the most effective ways to reduce the disease burden." The 2011 European Psychiatric Association (EPA) guidance on prevention of mental disorders states "There is considerable evidence that various psychiatric conditions can be prevented through the implementation of effective evidence-based interventions." A 2011 UK Department of Health report on the economic case for mental health promotion and mental illness prevention found that "many interventions are outstandingly good value for money, low in cost and often become self-financing over time, saving public expenditure". In 2016, the National Institute of Mental Health re-affirmed prevention as a research priority area.
Suicide and trauma is the increased risk of suicide that is caused by psychological trauma.

Suicide cases have remained constant or decreased since the outbreak of the COVID-19 pandemic. According to a study done on twenty-one high and upper-middle-income countries in April–July 2020, the number of suicides has remained static. These results were attributed to a variety of factors, including the composition of mental health support, financial assistance, having families and communities work diligently to care for at-risk individuals, discovering new ways to connect through the use of technology, and having more time spent with family members which aided in the strengthening of their bonds. Despite this, there has been an increase in isolation, fear, stigma, abuse, and economic fallout as a result of COVID-19. Self-reported levels of depression, anxiety, and suicidal thoughts were elevated during the initial stay-at-home periods, according to empirical evidence from several countries, but this does not appear to have translated into an increase in suicides.
Youth suicide in India is when young Indian people deliberately end their own life. People aged 15 to 24 years have the highest suicide rate in India, which is consistent with international trends in youth suicide. 35% of recorded suicides in India occur in this age group. Risk factors and methods of youth suicide differ from those in other age groups.