Vascular resistance is the resistance that must be overcome to push blood through the circulatory system and create blood flow. The resistance offered by the systemic circulation is known as the systemic vascular resistance (SVR) or may sometimes be called by the older term total peripheral resistance (TPR), while the resistance offered by the pulmonary circulation is known as the pulmonary vascular resistance (PVR). Systemic vascular resistance is used in calculations of blood pressure, blood flow, and cardiac function. Vasoconstriction (i.e., decrease in blood vessel diameter) increases SVR, whereas vasodilation (increase in diameter) decreases SVR.
Units for measuring vascular resistance are dyn·s·cm−5, pascal seconds per cubic metre (Pa·s/m3) or, for ease of deriving it by pressure (measured in mmHg) and cardiac output (measured in L/min), it can be given in mmHg·min/L. This is numerically equivalent to hybrid resistance units (HRU), also known as Wood units (in honor of Paul Wood, an early pioneer in the field), frequently used by pediatric cardiologists. The conversion between these units is:[1]
The basic tenet of calculating resistance is that flow is equal to driving pressure divided by flow rate.[citation needed]
where
R is Resistance
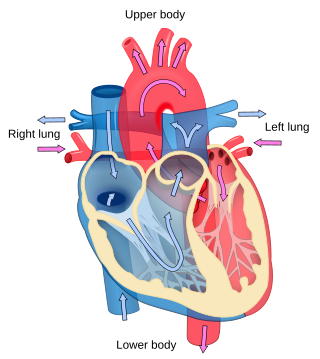
ΔP is the change in pressure across the circulation loop (systemic / pulmonary) from its beginning (immediately after exiting the left ventricle / right ventricle) to its end (entering the right atrium / left atrium)
Q is the flow through the vasculature (when discussing SVR this is equal to cardiac output)
This is the hydraulic version of Ohm's law, V=IR (which can be restated as R=V/I), in which the pressure differential is analogous to the electrical voltage drop, flow is analogous to electric current, and vascular resistance is analogous to electrical resistance.
Systemic calculations
The systemic vascular resistance can therefore be calculated in units of dyn·s·cm−5 as
where mean arterial pressure is 2/3 of diastolic blood pressure plus 1/3 of systolic blood pressure [or Diastolic + 1/3(Systolic-Diastolic)].
Mean arterial pressure is most commonly measured using a sphygmomanometer, and calculating a specialized average between systolic and diastolic blood pressures. Venous pressure, also known as central venous pressure, is measured at the right atrium and is usually very low (normally around 4mm Hg). As a result, it is sometimes disregarded.[citation needed]
It is difficult to measure or monitor SVR in most locations outside the ICU. An invasive catheter is necessary. SVR, BP and CO are related to each other but only BP is easily measured. In the typical situation at the bedside we have an equation with three variables, one known, that is the BP and two unknown, CO and SVR. For this reason the BP is frequently used as a practical but somewhat inadequate definition of Shock or the state of blood flow.
Pulmonary calculations
The pulmonary vascular resistance can be calculated in units of dyn·s·cm−5 as[citation needed]
where the pressures are measured in units of millimetres of mercury (mmHg) and the cardiac output is measured in units of litres per minute (L/min). The pulmonary artery wedge pressure (also called pulmonary artery occlusion pressure or PAOP) is a measurement in which one of the pulmonary arteries is occluded, and the pressure downstream from the occlusion is measured in order to approximately sample the left atrial pressure.[4] Therefore, the numerator of the above equation is the pressure difference between the input to the pulmonary blood circuit (where the heart's right ventricle connects to the pulmonary trunk) and the output of the circuit (which is the input to the left atrium of the heart). The above equation contains a numerical constant to compensate for the units used, but is conceptually equivalent to the following:[citation needed]
where R is the pulmonary vascular resistance (fluid resistance), ΔP is the pressure difference across the pulmonary circuit, and Q is the rate of blood flow through it.
As an example: If Systolic pressure: 120 mmHg, Diastolic pressure: 80 mmHg, Right atrial mean pressure: 3 mmHg, Cardiac output: 5 L/min, Then mean arterial pressure would be: (2 diastolic pressure + systolic pressure)/3 = 93.3 mmHg, and systemic vascular resistance: (93 - 3) / 5 = 18 Wood units, or equivalently 1440 dyn·s/cm5.
In a first approach, based on fluids dynamics (where the flowing material is continuous and made of continuous atomic or molecular bonds, the internal friction happen between continuous parallel layers of different velocities) factors that influence vascular resistance are represented in an adapted form of the Hagen–Poiseuille equation:[citation needed]
Vessel length is generally not subject to change in the body.
In Hagen–Poiseuille equation, the flow layers start from the wall and, by viscosity, reach each other in the central line of the vessel following a parabolic velocity profile.[citation needed]
In a second approach, more realistic and coming from experimental observations on blood flows, according to Thurston,[5] there is a plasma release-cell layering at the walls surrounding a plugged flow. It is a fluid layer in which at a distance δ, viscosity η is a function of δ written as η(δ), and these surrounding layers do not meet at the vessel centre in real blood flow. Instead, there is the plugged flow which is hyperviscous because holding high concentration of RBCs. Thurston assembled this layer to the flow resistance to describe blood flow by means of a viscosity η(δ) and thickness δ from the wall layer.[citation needed]
The blood resistance law appears as R adapted to blood flow profile:
η(δ) = viscosity of blood in the wall plasma release-cell layering
r = radius of the blood vessel
δ = distance in the plasma release-cell layer
Blood resistance varies depending on blood viscosity and its plugged flow (or sheath flow since they are complementary across the vessel section) size as well, and on the size of the vessels.
Blood viscosity increases as blood is more hemoconcentrated, and decreases as blood is more dilute. The greater the viscosity of blood, the larger the resistance will be. In the body, blood viscosity increases as red blood cell concentration increases, thus more hemodilute blood will flow more readily, while more hemoconcentrated blood will flow more slowly.[citation needed]
Counteracting this effect, decreased viscosity in a liquid results in the potential for increased turbulence. Turbulence can be viewed from outside of the closed vascular system as increased resistance, thereby countering the ease of flow of more hemodilute blood. Turbulence, particularly in large vessels, may account for some pressure change across the vascular bed.
The major regulator of vascular resistance in the body is regulation of vessel radius. In humans, there is very little pressure change as blood flows from the aorta to the large arteries, but the small arteries and arterioles are the site of about 70% of the pressure drop, and are the main regulators of SVR. When environmental changes occur (e.g. exercise, immersion in water), neuronal and hormonal signals, including binding of norepinephrine and epinephrine to the α1 receptor on vascular smooth muscles, cause either vasoconstriction or vasodilation. Because resistance is inversely proportional to the fourth power of vessel radius, changes to arteriole diameter can result in large increases or decreases in vascular resistance.[6]
If the resistance is inversely proportional to the fourth power of vessel radius, the resulting force exerted on the wall vessels, the parietal drag force, is inversely proportional to the second power of the radius. The force exerted by the blood flow on the vessel walls is, according to the Poiseuille equation, the wall shear stress. This wall shear stress is proportional to the pressure drop. The pressure drop is applied on the section surface of the vessel, and the wall shear stress is applied on the sides of the vessel. So the total force on the wall is proportional to the pressure drop and the second power of the radius. Thus the force exerted on the wall vessels is inversely proportional to the second power of the radius.
The blood flow resistance in a vessel is mainly regulated by the vessel radius and viscosity when blood viscosity too varies with the vessel radius. According to very recent results showing the sheath flow surrounding the plug flow in a vessel,[7] the sheath flow size is not neglectible in the real blood flow velocity profile in a vessel. The velocity profile is directly linked to flow resistance in a vessel. The viscosity variations, according to Thurston,[5] are also balanced by the sheath flow size around the plug flow. The secondary regulators of vascular resistance, after vessel radius, is the sheath flow size and its viscosity.
Thurston,[5] as well, shows that the resistance R is constant, where, for a defined vessel radius, the value η(δ)/δ is constant in the sheath flow.
Vascular resistance depends on blood flow which is divided into 2 adjacent parts: a plug flow, highly concentrated in RBCs, and a sheath flow, more fluid plasma release-cell layering. Both coexist and have different viscosities, sizes and velocity profiles in the vascular system.[citation needed]
Combining Thurston's work with the Hagen-Poiseuille equation shows that blood flow exerts a force on vessel walls which is inversely proportional to the radius and the sheath flow thickness. It is proportional to the mass flow rate and blood viscosity.
η(δ) = dynamic viscosity of blood in the wall plasma release-cell layering
r = radius of the blood vessel
δ = distance in the plasma release-cell layer or sheath flow thickness
Other factors
Many of the platelet-derived substances, including serotonin, are vasodilatory when the endothelium is intact and are vasoconstrictive when the endothelium is damaged.[citation needed]
Cholinergic stimulation causes release of endothelium-derived relaxing factor (EDRF) (later it was discovered that EDRF was nitric oxide) from intact endothelium, causing vasodilation. If the endothelium is damaged, cholinergic stimulation causes vasoconstriction.[8]
Adenosine most likely does not play a role in maintaining the vascular resistance in the resting state. However, it causes vasodilation and decreased vascular resistance during hypoxia. Adenosine is formed in the myocardial cells during hypoxia, ischemia, or vigorous work, due to the breakdown of high-energy phosphate compounds (e.g., adenosine monophosphate, AMP). Most of the adenosine that is produced leaves the cell and acts as a direct vasodilator on the vascular wall. Because adenosine acts as a direct vasodilator, it is not dependent on an intact endothelium to cause vasodilation.[citation needed]
Adenosine causes vasodilation in the small and medium-sized resistance arterioles (less than 100μm in diameter). When adenosine is administered it can cause a coronary steal phenomenon,[9] where the vessels in healthy tissue dilate more than diseased vessels. When this happens blood is shunted from potentially ischemic tissue that can now become ischemic tissue. This is the principle behind adenosine stress testing. Adenosine is quickly broken down by adenosine deaminase, which is present in red cells and the vessel wall.[10] The coronary steal and the stress test can be quickly terminated by stopping the adenosine infusion.
Systemic
A decrease in SVR (e.g., during exercising) will result in an increased flow to tissues and an increased venous flow back to the heart. An increased SVR, as occurs with some medications, will decrease flow to tissues and decrease venous flow back to the heart. Vasoconstriction and an increased SVR is particularly true of drugs the stimulate alpha(1) adrenergic receptors.[11][12]
Pulmonary
The major determinant of vascular resistance is small arteriolar (known as resistance arterioles) tone. These vessels are from 450 μm down to 100μm in diameter (as a comparison, the diameter of a capillary is about 5 to 10μm). Another determinant of vascular resistance is the pre-capillary arterioles. These arterioles are less than 100μm in diameter. They are sometimes known as autoregulatory vessels since they can dynamically change in diameter to increase or reduce blood flow.[citation needed]
Any change in the viscosity of blood (such as due to a change in hematocrit) would also affect the measured vascular resistance.[citation needed]
Pulmonary vascular resistance (PVR) also depends on the lung volume, and PVR is lowest at the functional residual capacity (FRC). The highly compliant nature of the pulmonary circulation means that the degree of lung distention has a large effect on PVR. This results primarily due to effects on the alveolar and extra-alveolar vessels. During inspiration, increased lung volumes cause alveolar expansion and lengthwise stretching of the interstitial alveolar vessels. This increases their length and reduces their diameter, thus increasing alveolar vessel resistance. On the other hand, decreased lung volumes during expiration cause the extra-alveolar arteries and veins to become narrower due to decreased radial traction from adjacent tissues. This leads to an increase in extra-alveolar vessel resistance. PVR is calculated as a sum of the alveolar and extra-alveolar resistances as these vessels lie in series with each other. Because the alveolar and extra-alveolar resistances are increased at high and low lung volumes respectively, the total PVR takes the shape of a U curve. The point at which PVR is the lowest is near the FRC.[citation needed]
Coronary
The regulation of tone in the coronary arteries is a complex subject. There are a number of mechanisms for regulating coronary vascular tone, including metabolic demands (i.e. hypoxia), neurologic control, and endothelial factors (i.e. EDRF, endothelin).[citation needed]
Local metabolic control (based on metabolic demand) is the most important mechanism of control of coronary flow. Decreased tissue oxygen content and increased tissue CO2 content act as vasodilators. Acidosis acts as a direct coronary vasodilator and also potentiates the actions of adenosine on the coronary vasculature.[citation needed]
Cardiology is the study of the heart. Cardiology is a branch of medicine that deals with disorders of the heart and the cardiovascular system. The field includes medical diagnosis and treatment of congenital heart defects, coronary artery disease, heart failure, valvular heart disease, and electrophysiology. Physicians who specialize in this field of medicine are called cardiologists, a specialty of internal medicine. Pediatric cardiologists are pediatricians who specialize in cardiology. Physicians who specialize in cardiac surgery are called cardiothoracic surgeons or cardiac surgeons, a specialty of general surgery.
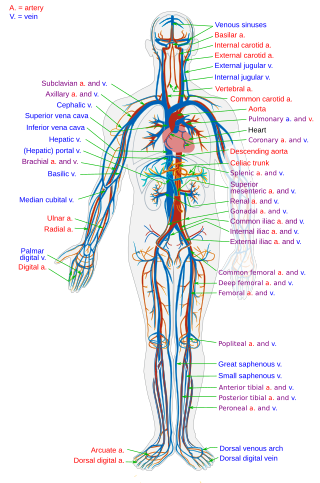
Blood vessels are the components of the circulatory system that transport blood throughout the human body. These vessels transport blood cells, nutrients, and oxygen to the tissues of the body. They also take waste and carbon dioxide away from the tissues. Blood vessels are needed to sustain life, because all of the body's tissues rely on their functionality.
Blood pressure (BP) is the pressure of circulating blood against the walls of blood vessels. Most of this pressure results from the heart pumping blood through the circulatory system. When used without qualification, the term "blood pressure" refers to the pressure in a brachial artery, where it is most commonly measured. Blood pressure is usually expressed in terms of the systolic pressure over diastolic pressure in the cardiac cycle. It is measured in millimeters of mercury (mmHg) above the surrounding atmospheric pressure, or in kilopascals (kPa). The difference between the systolic and diastolic pressures is known as pulse pressure, while the average pressure during a cardiac cycle is known as mean arterial pressure.
Hemodynamics or haemodynamics are the dynamics of blood flow. The circulatory system is controlled by homeostatic mechanisms of autoregulation, just as hydraulic circuits are controlled by control systems. The hemodynamic response continuously monitors and adjusts to conditions in the body and its environment. Hemodynamics explains the physical laws that govern the flow of blood in the blood vessels.
Vasoconstriction is the narrowing of the blood vessels resulting from contraction of the muscular wall of the vessels, in particular the large arteries and small arterioles. The process is the opposite of vasodilation, the widening of blood vessels. The process is particularly important in controlling hemorrhage and reducing acute blood loss. When blood vessels constrict, the flow of blood is restricted or decreased, thus retaining body heat or increasing vascular resistance. This makes the skin turn paler because less blood reaches the surface, reducing the radiation of heat. On a larger level, vasoconstriction is one mechanism by which the body regulates and maintains mean arterial pressure.
Vasodilation, also known as vasorelaxation, is the widening of blood vessels. It results from relaxation of smooth muscle cells within the vessel walls, in particular in the large veins, large arteries, and smaller arterioles. Blood vessel walls are composed of endothelial tissue and a basal membrane lining the lumen of the vessel, concentric smooth muscle layers on top of endothelial tissue, and an adventitia over the smooth muscle layers. Relaxation of the smooth muscle layer allows the blood vessel to dilate, as it is held in a semi-constricted state by sympathetic nervous system activity. Vasodilation is the opposite of vasoconstriction, which is the narrowing of blood vessels.
An arteriole is a small-diameter blood vessel in the microcirculation that extends and branches out from an artery and leads to capillaries.
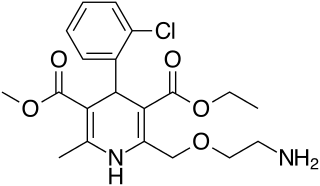
Amlodipine, sold under the brand name Norvasc among others, is a calcium channel blocker medication used to treat high blood pressure, coronary artery disease (CAD) and variant angina. It is taken orally.
Compliance is the ability of a hollow organ (vessel) to distend and increase volume with increasing transmural pressure or the tendency of a hollow organ to resist recoil toward its original dimensions on application of a distending or compressing force. It is the reciprocal of "elastance", hence elastance is a measure of the tendency of a hollow organ to recoil toward its original dimensions upon removal of a distending or compressing force.
Cardiac catheterization is the insertion of a catheter into a chamber or vessel of the heart. This is done both for diagnostic and interventional purposes.
Aerospace physiology is the study of the effects of high altitudes on the body, such as different pressures and levels of oxygen. At different altitudes the body may react in different ways, provoking more cardiac output, and producing more erythrocytes. These changes cause more energy waste in the body, causing muscle fatigue, but this varies depending on the level of the altitude.
Hyperaemia is the increase of blood flow to different tissues in the body. It can have medical implications but is also a regulatory response, allowing change in blood supply to different tissues through vasodilation. Clinically, hyperaemia in tissues manifests as erythema because of the engorgement of vessels with oxygenated blood. Hyperaemia can also occur due to a fall in atmospheric pressure outside the body. The term comes from Greek ὑπέρ (hupér) 'over', and αἷμα (haîma) 'blood'.
Portopulmonary hypertension (PPH) is defined by the coexistence of portal and pulmonary hypertension. PPH is a serious complication of liver disease, present in 0.25 to 4% of all patients with cirrhosis. Once an absolute contraindication to liver transplantation, it is no longer, thanks to rapid advances in the treatment of this condition. Today, PPH is comorbid in 4-6% of those referred for a liver transplant.
The Womersley number is a dimensionless number in biofluid mechanics and biofluid dynamics. It is a dimensionless expression of the pulsatile flow frequency in relation to viscous effects. It is named after John R. Womersley (1907–1958) for his work with blood flow in arteries. The Womersley number is important in keeping dynamic similarity when scaling an experiment. An example of this is scaling up the vascular system for experimental study. The Womersley number is also important in determining the thickness of the boundary layer to see if entrance effects can be ignored.
In respiratory physiology, airway resistance is the resistance of the respiratory tract to airflow during inhalation and exhalation. Airway resistance can be measured using plethysmography.
The zones of the lung divide the lung into four vertical regions, based upon the relationship between the pressure in the alveoli (PA), in the arteries (Pa), in the veins (Pv) and the pulmonary interstitial pressure (Pi):
Persistent fetal circulation is a condition caused by a failure in the systemic circulation and pulmonary circulation to convert from the antenatal circulation pattern to the "normal" pattern. Infants experience a high mean arterial pulmonary artery pressure and a high afterload at the right ventricle. This means that the heart is working against higher pressures, which makes it more difficult for the heart to pump blood.
Coronary perfusion pressure (CPP) refers to the pressure gradient that drives coronary blood pressure. The heart's function is to perfuse blood to the body; however, the heart's own myocardium must, itself, be supplied for its own muscle function. The heart is supplied by coronary vessels, and therefore CPP is the blood pressure within those vessels. If pressures are too low in the coronary vasculature, then the myocardium risks ischemia with subsequent myocardial infarction or cardiogenic shock.
Microvasculature comprises the microvessels – venules and capillaries of the microcirculation, with a maximum average diameter of 0.3 millimeters. As the vessels decrease in size, they increase their surface-area-to-volume ratio. This allows surface properties to play a significant role in the function of the vessel.
In physiology, acute local blood flow regulation refers to an intrinsic regulation, or control, of the vascular tone of arteries at a local level, meaning within a certain tissue type, organ, or organ system. This intrinsic type of control means that the blood vessels can automatically adjust their own vascular tone, by dilating (widening) or constricting (narrowing), in response to some change in the environment. This change occurs in order to match up the tissue's oxygen demand with the actual oxygen supply available in the blood as closely as possible. For example, if a muscle is being utilized actively, it will require more oxygen than it was at rest, so the blood vessels supplying that muscle will vasodilate, or widen in size, to increase the amount of blood, and therefore oxygen, being delivered to that muscle.
References
↑ Fuster, V.; Alexander, R.W.; O'Rourke, R.A. (2004) Hurst's the heart, book 1. 11th Edition, McGraw-Hill Professional, Medical Pub. Division. Page 513. ISBN978-0-07-143224-5.
1 2 Table 30-1 in: Trudie A Goers; Washington University School of Medicine Department of Surgery; Klingensmith, Mary E; Li Ern Chen; Sean C Glasgow (2008). The Washington manual of surgery. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN978-0-7817-7447-5.{{cite book}}: CS1 maint: multiple names: authors list (link)
↑ Measurement of real pulsatile blood flow using X-ray PIV technique with CO2 microbubbles, Hanwook Park, Eunseop Yeom, Seung-Jun Seo, Jae-Hong Lim & Sang-Joon Lee, NATURE, Scientific Reports5, Article number: 8840 (2015), doi:10.1038/srep08840.
↑ Masugata H, Peters B, Lafitte S, etal. (2003). "Assessment of adenosine-induced coronary steal in the setting of coronary occlusion based on the extent of opacification defects by myocardial contrast echocardiography". Angiology. 54 (4): 443–8. doi:10.1177/000331970305400408. PMID12934764. S2CID42646704.
↑ Robert F. Brooker, John F. IV Butterworth, Dalane W. Kitzman, Jeffrey M. Berman, Hillel I. Kashtan, A. Colin McKinley; Treatment of Hypotension after Hyperbaric Tetracaine Spinal Anesthesia: A Randomized, Double-blind, Cross-over Comparison of Phenylephrine and Epinephrine. Anesthesiology 1997; 86:797–805 doi:10.1097/00000542-199704000-00009
Further reading
Grossman W, Baim D. Grossman'sCardiac Catheterization, Angiography, and Intervention, Sixth Edition. Page 172, Tabe 8.1 ISBN0-683-30741-X
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.