
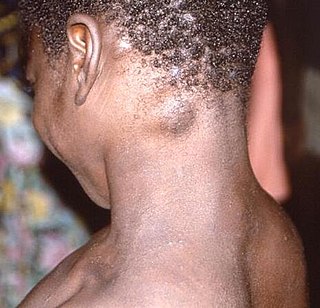
Mpox is an infectious viral disease that can occur in humans and other animals. Symptoms include a rash that forms blisters and then crusts over, fever, and swollen lymph nodes. The illness is usually mild, and most infected individuals recover within a few weeks without treatment. The time from exposure to the onset of symptoms ranges from three to seventeen days, and symptoms typically last from two to four weeks. However, cases may be severe, especially in children, pregnant women, or people with suppressed immune systems.

Influenza A virus subtype H5N1 (A/H5N1) is a subtype of the influenza A virus, which causes influenza (flu), predominantly in birds. It is enzootic in many bird populations, and also panzootic. A/H5N1 virus can also infect mammals that have been exposed to infected birds; in these cases, symptoms are frequently severe or fatal.

Health problems have been a long-standing issue limiting development in the Democratic Republic of the Congo.

Kwango is a province of the Democratic Republic of the Congo. It is one of the 21 provinces created in the 2015 repartitioning. Kwango, Kwilu, and Mai-Ndombe provinces are the result of the dismemberment of the former Bandundu province. Kwango was formed from the Kwango district whose town of Kenge was made the provincial capital and thus gained city status.

Ebola, also known as Ebola virus disease (EVD) and Ebola hemorrhagic fever (EHF), is a viral hemorrhagic fever in humans and other primates, caused by ebolaviruses. Symptoms typically start anywhere between two days and three weeks after infection. The first symptoms are usually fever, sore throat, muscle pain, and headaches. These are usually followed by vomiting, diarrhoea, rash and decreased liver and kidney function, at which point some people begin to bleed both internally and externally. It kills between 25% and 90% of those infected – about 50% on average. Death is often due to shock from fluid loss, and typically occurs between six and 16 days after the first symptoms appear. Early treatment of symptoms increases the survival rate considerably compared to late start. An Ebola vaccine was approved by the US FDA in December 2019.
In 2014, an outbreak of Ebola virus disease in the Democratic Republic of the Congo (DRC) occurred. Genome sequencing has shown that this outbreak was not related to the 2014–15 West Africa Ebola virus epidemic, but was of the same EBOV species. It began in August 2014 and was declared over in November of that year, after 42 days without any new cases. This is the 7th outbreak there, three of which occurred during the period of Zaire.

On 11 May 2017, the Democratic Republic of the Congo (DRC) was identified by the World Health Organization (WHO) as having one Ebola-related death.

The 2018 Équateur province Ebola outbreak occurred in the north-west of the Democratic Republic of the Congo (DRC) from May to July 2018. It was contained entirely within Équateur province, and was the first time that vaccination with the rVSV-ZEBOV Ebola vaccine had been attempted in the early stages of an Ebola outbreak, with a total of 3,481 people vaccinated. It was the ninth recorded Ebola outbreak in the DRC.
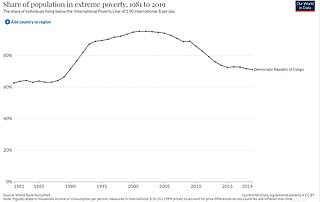
Poverty is widespread and unchecked across the 26 provinces of the Democratic Republic of the Congo (DRC). Despite being the second-largest country in Africa, with an approximate area of 2.3 million square kilometres (890,000 sq mi), and being endowed with rich natural resources, the DRC is the second-poorest country in the world. The average annual income is only $449 US dollars. In 2019, the United Nations (UN) Human Development Index (HDI) ranked the DRC as the 175th least-developed country out of 189 countries with an HDI of 0.480. In 2023, almost 75% of Congolese people live on less than $2.15 a day, defined as the threshold for extreme poverty.

The Kivu Ebola epidemic was an outbreak of Ebola virus disease (EVD) mainly in eastern Democratic Republic of the Congo (DRC), and in other parts of Central Africa, from 2018 to 2020. Between 1 August 2018 and 25 June 2020 it resulted in 3,470 reported cases. The Kivu outbreak also affected Ituri Province, whose first case was confirmed on 13 August 2018. In November 2018, the outbreak became the biggest Ebola outbreak in the DRC's history, and had become the second-largest Ebola outbreak in recorded history worldwide, behind only the 2013–2016 Western Africa epidemic. In June 2019, the virus reached Uganda, having infected a 5-year-old Congolese boy who entered Uganda with his family, but was contained.

Jean-Jacques Muyembe is a Congolese microbiologist. He is the general director of the Democratic Republic of the Congo Institut National pour la Recherche Biomedicale (INRB). He was part of team at the Yambuku Catholic Mission Hospital that investigated the first Ebola outbreak, and was part of the effort that discovered Ebola as a new disease, although his exact role is still subject to controversy. In 2016, he led the research that designed, along with other researchers at the INRB and the National Institute of Health Vaccine Research Center in the US, one of the most promising treatment for Ebola, mAb114. The treatment was successfully tested during recent outbreaks in the DRC, on the express decision of the then DRC Minister of Health, Dr Oly Ilunga, despite advice against this from the World Health Organization.

In 2019, a measles epidemic broke out in the Democratic Republic of the Congo (DRC). The epidemic started in early 2019 in the southeast corner of the DRC and then spread to all provinces. By June 2019 the epidemic was reported to have exceeded the death toll of the concurrent Ebola epidemic. By April 2020, it had infected more than 341,000 people and claimed about 6,400 fatalities. This has primarily affected children under the age of five, representing 74% of infections and nearly 90% of deaths.
The COVID-19 pandemic in the Democratic Republic of the Congo was a part of the worldwide pandemic of coronavirus disease 2019 caused by severe acute respiratory syndrome coronavirus 2. The virus was confirmed to have reached the Democratic Republic of the Congo on 10 March 2020. The first few confirmed cases were all outside arrivals.
In August–November 1976, an outbreak of Ebola virus disease occurred in Zaire. The first recorded case was from Yambuku, a small village in Mongala District, 1,098 kilometres (682 mi) northeast of the capital city of Kinshasa.

On 7 February 2021, the Congolese health ministry announced that a new case of Ebola near Butembo, North Kivu had been detected the previous day. The case was a 42-year-old woman who had symptoms of Ebola in Biena on 1 February 2021. A few days after, she died in a hospital in Butembo. The WHO said that more than 70 people who had contact with the woman had been tracked.
Mpox is endemic in western and central Africa, with the overwhelming majority of cases occurring in the Democratic Republic of the Congo (DRC), where the more virulent clade Ib has seen a rapid rise in infections since September 2023.
Events of the year 2024 in the Democratic Republic of the Congo.

An epidemic of a new variant of clade I mpox, called clade 1b, began in Central Africa at least as early as September 2023. As of September 2024, more than 29,000 cases have been reported, with over 800 fatalities, nearly all in the Democratic Republic of the Congo. According to the European CDC: "The size of these outbreaks could be larger than reported due to under-ascertainment and under-reporting."
This article documents the chronology and epidemiology of the 2023–2024 mpox epidemic, an outbreak of clade Ib of mpox.
