Related Research Articles

The trachea, also known as the windpipe, is a cartilaginous tube that connects the larynx to the bronchi of the lungs, allowing the passage of air, and so is present in almost all animals with lungs. The trachea extends from the larynx and branches into the two primary bronchi. At the top of the trachea the cricoid cartilage attaches it to the larynx. The trachea is formed by a number of horseshoe-shaped rings, joined together vertically by overlying ligaments, and by the trachealis muscle at their ends. The epiglottis closes the opening to the larynx during swallowing.

Tracheal intubation, usually simply referred to as intubation, is the placement of a flexible plastic tube into the trachea (windpipe) to maintain an open airway or to serve as a conduit through which to administer certain drugs. It is frequently performed in critically injured, ill, or anesthetized patients to facilitate ventilation of the lungs, including mechanical ventilation, and to prevent the possibility of asphyxiation or airway obstruction.
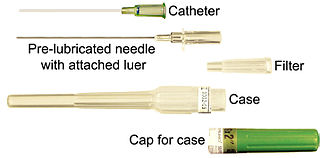
In medicine, a catheter (/ˈkæθətər/) is a thin tube made from medical grade materials serving a broad range of functions. Catheters are medical devices that can be inserted in the body to treat diseases or perform a surgical procedure. Catheters are manufactured for specific applications, such as cardiovascular, urological, gastrointestinal, neurovascular and ophthalmic procedures. The process of inserting a catheter is catheterization.

A bronchus is a passage or airway in the lower respiratory tract that conducts air into the lungs. The first or primary bronchi to branch from the trachea at the carina are the right main bronchus and the left main bronchus. These are the widest bronchi, and enter the right lung, and the left lung at each hilum. The main bronchi branch into narrower secondary bronchi or lobar bronchi, and these branch into narrower tertiary bronchi or segmental bronchi. Further divisions of the segmental bronchi are known as 4th order, 5th order, and 6th order segmental bronchi, or grouped together as subsegmental bronchi. The bronchi, when too narrow to be supported by cartilage, are known as bronchioles. No gas exchange takes place in the bronchi.

Pulmonary aspiration is the entry of material such as pharyngeal secretions, food or drink, or stomach contents from the oropharynx or gastrointestinal tract, into the larynx and lower respiratory tract, the portions of the respiratory system from the trachea (windpipe) to the lungs. A person may inhale the material, or it may be delivered into the tracheobronchial tree during positive pressure ventilation. When pulmonary aspiration occurs during eating and drinking, the aspirated material is often colloquially referred to as "going down the wrong pipe".

Laryngoscopy is endoscopy of the larynx, a part of the throat. It is a medical procedure that is used to obtain a view, for example, of the vocal folds and the glottis. Laryngoscopy may be performed to facilitate tracheal intubation during general anaesthesia or cardiopulmonary resuscitation or for surgical procedures on the larynx or other parts of the upper tracheobronchial tree.
A tracheal tube is a catheter that is inserted into the trachea for the primary purpose of establishing and maintaining a patent airway and to ensure the adequate exchange of oxygen and carbon dioxide.
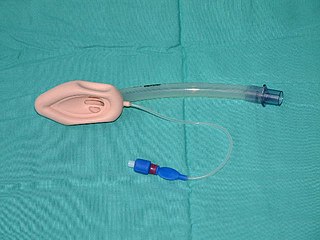
A laryngeal mask airway (LMA), also known as laryngeal mask, is a medical device that keeps a patient's airway open during anaesthesia or while they are unconscious. It is a type of supraglottic airway device. They are most commonly used by anaesthetists to channel oxygen or inhalational anaesthetic to the lungs during surgery and in the pre-hospital setting for unconscious patients.

Falloposcopy is the inspection of the fallopian tubes through a micro- endoscope. The falloposcope is inserted into the tube through its opening in the uterus at the proximal tubal opening via the uterotubal junction; technically it could also be inserted at the time of abdominal surgery or laparoscopy via the distal fimbriated end.

Flail chest is a life-threatening medical condition that occurs when a segment of the rib cage breaks due to trauma and becomes detached from the rest of the chest wall. Two of the symptoms of flail chest are chest pain and shortness of breath.

The Combitube—also known as the esophageal tracheal airway or esophageal tracheal double-lumen airway—is a blind insertion airway device (BIAD) used in the pre-hospital and emergency setting. It is designed to provide an airway to facilitate the mechanical ventilation of a patient in respiratory distress.

Bronchoscopy is an endoscopic technique of visualizing the inside of the airways for diagnostic and therapeutic purposes. An instrument (bronchoscope) is inserted into the airways, usually through the nose or mouth, or occasionally through a tracheostomy. This allows the practitioner to examine the patient's airways for abnormalities such as foreign bodies, bleeding, tumors, or inflammation. Specimens may be taken from inside the lungs. The construction of bronchoscopes ranges from rigid metal tubes with attached lighting devices to flexible optical fiber instruments with realtime video equipment.
Cardiothoracic anesthesiology is a subspeciality of the medical practice of anesthesiology, devoted to the preoperative, intraoperative, and postoperative care of adult and pediatric patients undergoing cardiothoracic surgery and related invasive procedures.

Tracheobronchial injury is damage to the tracheobronchial tree. It can result from blunt or penetrating trauma to the neck or chest, inhalation of harmful fumes or smoke, or aspiration of liquids or objects.
Tracheal intubation, an invasive medical procedure, is the placement of a flexible plastic catheter into the trachea. For millennia, tracheotomy was considered the most reliable method of tracheal intubation. By the late 19th century, advances in the sciences of anatomy and physiology, as well as the beginnings of an appreciation of the germ theory of disease, had reduced the morbidity and mortality of this operation to a more acceptable rate. Also in the late 19th century, advances in endoscopic instrumentation had improved to such a degree that direct laryngoscopy had finally become a viable means to secure the airway by the non-surgical orotracheal route. Nasotracheal intubation was not widely practiced until the early 20th century. The 20th century saw the transformation of the practices of tracheotomy, endoscopy and non-surgical tracheal intubation from rarely employed procedures to essential components of the practices of anesthesia, critical care medicine, emergency medicine, gastroenterology, pulmonology and surgery.

Brachial plexus block is a regional anesthesia technique that is sometimes employed as an alternative or as an adjunct to general anesthesia for surgery of the upper extremity. This technique involves the injection of local anesthetic agents in close proximity to the brachial plexus, temporarily blocking the sensation and ability to move the upper extremity. The subject can remain awake during the ensuing surgical procedure, or they can be sedated or even fully anesthetized if necessary.

Foreign body aspiration occurs when a foreign body enters the airway which can cause difficulty breathing or choking. Objects may reach the respiratory tract and the digestive tract from the mouth and nose, but when an object enters the respiratory tract it is termed aspiration. The foreign body can then become lodged in the trachea or further down the respiratory tract such as in a bronchus. Regardless of the type of object, any aspiration can be a life-threatening situation and requires timely recognition and action to minimize risk of complications. While advances have been made in management of this condition leading to significantly improved clinical outcomes, there were still 2,700 deaths resulting from foreign body aspiration in 2018. Approximately one child dies every five days due to choking on food in the United States, highlighting the need for improvements in education and prevention.
Tracheal agenesis is a rare birth defect with a prevalence of less than 1 in 50,000 in which the trachea fails to develop, resulting in an impaired communication between the larynx and the alveoli of the lungs. Although the defect is normally fatal, occasional cases have been reported of long-term survival following surgical intervention.

The laryngeal tube is an airway management device designed as an alternative to other airway management techniques such as mask ventilation, laryngeal mask airway, and tracheal intubation. This device can be inserted blindly through the oropharynx into the hypopharynx to create an airway during anaesthesia and cardiopulmonary resuscitation so as to enable mechanical ventilation of the lungs.

A double-lumen endotracheal tube is a type of endotracheal tube which is used in tracheal intubation during thoracic surgery and other medical conditions to achieve selective, one-sided ventilation of either the right or the left lung.
References
- 1 2 3 4 Brodsky, J. B. (11 December 2009). "Lung separation and the difficult airway". British Journal of Anaesthesia. 103 (Supplement 1): i66–i75. doi: 10.1093/bja/aep262 . PMID 20007992.
- ↑ Venkataraju, A; Rozario, C; Saravanan, P (April 2010). "Accidental fracture of the tip of the Coopdech bronchial blocker during insertion for one lung ventilation". Canadian Journal of Anesthesia. 57 (4): 350–4. doi: 10.1007/s12630-009-9261-0 . PMID 20049575.
- ↑ Ozaki, M; Murashima, K; Koga, K; Sata, T (April 2010). "Use of the Coopdech Bronchial Blocker as a tracheal tube introducer in a patient with difficult laryngoscopy". Journal of Anesthesia. 24 (2): 319–20. doi:10.1007/s00540-010-0890-9. PMID 20204422. S2CID 6945704.
- ↑ Mourisse, J.; Liesveld, J.; Verhagen, A.; van Rooij, G.; van der Heide, S.; Schuurbiers-Siebers, O.; Van der Heijden, E. (March 2013). "Efficiency, efficacy, and safety of EZ-blocker compared with left-sided double-lumen tube for one-lung ventilation". Anesthesiology. 118 (3): 550–61. doi: 10.1097/ALN.0b013e3182834f2d . PMID 23299364.