Related Research Articles
Diarrhea, also spelled diarrhoea or diarrhœa in British English, is the condition of having at least three loose, liquid, or watery bowel movements each day. It often lasts for a few days and can result in dehydration due to fluid loss. Signs of dehydration often begin with loss of the normal stretchiness of the skin and irritable behaviour. This can progress to decreased urination, loss of skin color, a fast heart rate, and a decrease in responsiveness as it becomes more severe. Loose but non-watery stools in babies who are exclusively breastfed, however, are normal.

Coeliac disease or celiac disease is a long-term autoimmune disorder, primarily affecting the small intestine, where individuals develop intolerance to gluten, present in foods such as wheat, rye and barley. Classic symptoms include gastrointestinal problems such as chronic diarrhoea, abdominal distention, malabsorption, loss of appetite, and among children failure to grow normally. This often begins between six months and two years of age. Non-classic symptoms are more common, especially in people older than two years. There may be mild or absent gastrointestinal symptoms, a wide number of symptoms involving any part of the body, or no obvious symptoms. Coeliac disease was first described in childhood; however, it may develop at any age. It is associated with other autoimmune diseases, such as Type 1 diabetes mellitus and Hashimoto's thyroiditis, among others.

Intrinsic factor (IF), cobalamin binding intrinsic factor, also known as gastric intrinsic factor (GIF), is a glycoprotein produced by the parietal cells (in humans) or chief cells (in rodents) of the stomach. It is necessary for the absorption of vitamin B12 later on in the distal ileum of the small intestine. In humans, the gastric intrinsic factor protein is encoded by the CBLIF gene. Haptocorrin (transcobalamin I) is another glycoprotein secreted by the salivary glands which binds to vitamin B12. Vitamin B12 is acid-sensitive and in binding to haptocorrin it can safely pass through the acidic stomach to the duodenum.
Enteritis is inflammation of the small intestine. It is most commonly caused by food or drink contaminated with pathogenic microbes, such as Serratia, but may have other causes such as NSAIDs, radiation therapy as well as autoimmune conditions like Crohn's disease and celiac disease. Symptoms include abdominal pain, cramping, diarrhea, dehydration, and fever. Related diseases of the gastrointestinal system include inflammation of the stomach and large intestine.
Malabsorption is a state arising from abnormality in absorption of food nutrients across the gastrointestinal (GI) tract. Impairment can be of single or multiple nutrients depending on the abnormality. This may lead to malnutrition and a variety of anaemias.

Small intestinal bacterial overgrowth (SIBO), also termed bacterial overgrowth, or small bowel bacterial overgrowth syndrome (SBBOS), is a disorder of excessive bacterial growth in the small intestine. Unlike the colon, which is rich with bacteria, the small bowel usually has fewer than 100,000 organisms per millilitre. Patients with bacterial overgrowth typically develop symptoms which may include nausea, bloating, vomiting, diarrhea, malnutrition, weight loss and malabsorption, which is caused by a number of mechanisms.
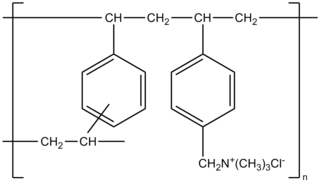
Colestyramine (INN) or cholestyramine (USAN) is a bile acid sequestrant, which binds bile in the gastrointestinal tract to prevent its reabsorption. It is a strong ion exchange resin, which means it can exchange its chloride anions with anionic bile acids in the gastrointestinal tract and bind them strongly in the resin matrix. The functional group of the anion exchange resin is a quaternary ammonium group attached to an inert styrene-divinylbenzene copolymer.

Microscopic colitis refers to two related medical conditions which cause diarrhea: collagenous colitis and lymphocytic colitis. Both conditions are characterized by the presence of chronic non-bloody watery diarrhea, normal appearances on colonoscopy and characteristic histopathology findings of inflammatory cells.

Lymphangiectasia, also known as "lymphangiectasis", is a pathologic dilation of lymph vessels. When it occurs in the intestines it is known as intestinal lymphangiectasia, colloquially recognized as Waldmann's disease in cases where there is no secondary cause. The primary defect lies in the inability of the lymphatic system to adequately drain lymph, resulting in its subsequent accumulation and leakage into the intestinal lumen. This condition, first described by Waldmann in 1961, is typically diagnosed in infancy or early childhood. However, it can also manifest in adults, exhibiting a broad spectrum of clinical symptoms.

Protein losing enteropathy is a syndrome of blood proteins being lost excessively via the gastrointestinal tract. It may be caused by many different underlying diseases that damage the lining of the GI tract (mucosa) or cause blockage of its lymphatic drainage.
Radiation enteropathy is a syndrome that may develop following abdominal or pelvic radiation therapy for cancer. Many affected people are cancer survivors who had treatment for cervical cancer or prostate cancer; it has also been termed pelvic radiation disease with radiation proctitis being one of the principal features.

Microvillus inclusion disease, previously known as Davidson's disease, congenital microvillus atrophy and, less specifically, microvillus atrophy, is a rare genetic disorder of the small intestine that is inherited in an autosomal recessive pattern.

Epithelial cell adhesion molecule (EpCAM), also known as CD326 among other names, is a transmembrane glycoprotein mediating Ca2+-independent homotypic cell–cell adhesion in epithelia. EpCAM is also involved in cell signaling, migration, proliferation, and differentiation. Additionally, EpCAM has oncogenic potential via its capacity to upregulate c-myc, e-fabp, and cyclins A & E. Since EpCAM is expressed exclusively in epithelia and epithelial-derived neoplasms, EpCAM can be used as diagnostic marker for various cancers. It appears to play a role in tumorigenesis and metastasis of carcinomas, so it can also act as a potential prognostic marker and as a potential target for immunotherapeutic strategies.

Tricho-hepato-enteric syndrome (THE), also known as syndromic or phenotypic diarrhea, is an extremely rare congenital bowel disorder which manifests itself as intractable diarrhea in infants with intrauterine growth retardation, hair and facial abnormalities. Many also have liver disease and abnormalities of the immune system. The associated malabsorption leads to malnutrition and failure to thrive.
Chronic diarrheaof infancy, also called toddler's diarrhea, is a common condition typically affecting up to 1.7 billion children between ages 6–30 months worldwide every year, usually resolving by age 4. According to the World Health Organization (WHO), diarrheal disease is the second greatest cause of death in children 5 years and younger. Diarrheal disease takes the lives of 525,000 or more children per year. Diarrhea is characterized as the condition of passing of three or more loose or watery bowel movements within a day sometimes with undigested food visible. Diarrhea is separated into three clinical categories; acute diarrhea may last multiple hours or days, acute bloody diarrhea, also known as dysentery, and finally, chronic or persistent diarrhea which lasts 2–4 weeks or more. There is normal growth with no evidence of malnutrition in the child experiencing persistent diarrhea. In chronic diarrhea there is no evidence of blood in the stool and there is no sign of infection. The condition may be related to irritable bowel syndrome. There are various tests that can be performed to rule out other causes of diarrhea that don't fall under the chronic criteria, including blood test, colonoscopy, and even genetic testing. Most acute or severe cases of diarrhea have treatment guidelines revolving around prescription or non prescription medications based on the cause, but the treatment protocols for chronic diarrhea focus on replenishing the body with lost fluids and electrolytes, because there typically isn't a treatable cause.
Bile acid malabsorption (BAM), known also as bile acid diarrhea, is a cause of several gut-related problems, the main one being chronic diarrhea. It has also been called bile acid-induced diarrhea, cholerheic or choleretic enteropathy, bile salt diarrhea or bile salt malabsorption. It can result from malabsorption secondary to gastrointestinal disease, or be a primary disorder, associated with excessive bile acid production. Treatment with bile acid sequestrants is often effective. It is recognised as a disability in the United Kingdom under the Equality Act 2010
Tetratricopeptide repeat domain 7A (TTC7A) is a protein that in humans is encoded by the TTC7A gene.

Autoimmune enteropathy is a rare autoimmune disorder characterized by weight loss from malabsorption, severe and protracted diarrhea, and autoimmune damage to the intestinal mucosa. Autoimmune enteropathy typically occurs in infants and younger children however, adult cases have been reported in literature. Autoimmune enteropathy was first described by Walker-Smith et al. in 1982.
Serum-derived bovine immunoglobulin/protein isolate (SBI) is a medical food product derived from bovine serum obtained from adult cows in the United States. It is sold under the name EnteraGam.
Duodenal lymphocytosis, sometimes called lymphocytic duodenitis, lymphocytic duodenosis, or duodenal intraepithelial lymphocytosis, is a condition where an increased number of intra-epithelial lymphocytes is seen in biopsies of the duodenal mucosa when these are examined microscopically. This form of lymphocytosis is often a feature of coeliac disease but may be found in other disorders.
References
- ↑ Sivagnanam, Mamata; Mueller, James L.; Lee, Hane; Chen, Zugen; Nelson, Stanley F.; Turner, Dan; Zlotkin, Stanley H.; Pencharz, Paul B.; Ngan, Bo-Yee; Libiger, Ondrej; Schork, Nicholas J.; Lavine, Joel E.; Taylor, Sharon; Newbury, Robert O.; Kolodner, Richard D.; Hoffman, Hal M. (May 15, 2008). "Identification of EpCAM as the gene for congenital tufting enteropathy". Gastroenterology. 135 (2): 429–347. doi:10.1053/j.gastro.2008.05.036. PMC 2574708 . PMID 18572020.
- ↑ Sivagnanam, M.; Janecke, A.R.; Müller, T.; Heinz-Erian, P.; Taylor, S; Bird, L.M. (2010). "Case of syndromic tufting enteropathy harbors SPINT2 mutation seen in congenital sodium diarrhea". Clinical Dysmorphology. 19 (1): 48. doi:10.1097/MCD.0b013e328331de38. PMC 6709868 . PMID 20009592.
- ↑ Salomon, J.; Espinosa-Parrilla, Y.; Goulet, O.; Al-Qabandi, W.; Guigue, P.; Canioni, D.; Bruneau, J.; Alzahrani, F.; Almuhsen, S.; Cerf-Bensussan, N.; Jeanpierre, M.; Brousse, N.; Lyonnet, S.; Munnich, A.; Smahi, A. (2008). "A founder effect at the EPCAM locus in Congenital Tufting Enteropathy in the Arabic Gulf". European Journal of Medical Genetics. 54 (3): 319–322. doi:10.1016/j.ejmg.2011.01.009. PMID 21315192.
- ↑ Goulet, O; Salomon, J; Ruemmele, F; Patey-Mariaud de Serres, N; Brousse, N (2007). "Intestinal epithelial dysplasia (tufting enteropathy)". Orphanet Journal of Rare Diseases. 2: 20. doi: 10.1186/1750-1172-2-20 . PMC 1878471 . PMID 17448233.
- ↑ Davidson, G.P.; Cutz, E.; Hamilton, J.R.; Gall, D.G. (1978). "Familial enteropathy: a syndrome of protracted diarrhea from birth, failure to thrive, and hypoplastic villus atrophy". Gastroenterology. 75 (5): 783–790. doi: 10.1016/0016-5085(78)90458-4 . PMID 100367..
- ↑ Reifen, R.M.; Cutz, E.; Griffiths, A-M.; Ngan, B.Y.; Sherman, P.M. (April 1994). "Tufting enteropathy: a newly recognized clinicopathological entity associated with refractory diarrhea in infants". Journal of Pediatric Gastroenterology and Nutrition. 18 (3): 379–385. doi: 10.1097/00005176-199404000-00022 . PMID 8057225.