Vaccination (such as for hepatitis B), avoiding alcohol,[1] losing weight, exercising, low-carbohydrate diet, controlling hypertension and diabetes may help in those with NAFLD or NASH
Cirrhosis, also known as liver cirrhosis, hepatic cirrhosis, chronic liver failure, chronic hepatic failure, and end-stage liver disease, is a chronic condition of the liver in which the normal functioning tissue, or parenchyma, is replaced with scar tissue (fibrosis) and regenerative nodules as a result of chronic liver disease.[6][7][8] Damage to the liver leads to repair of liver tissue and subsequent formation of scar tissue. Over time, scar tissue and nodules of regenerating hepatocytes can replace the parenchyma, causing increased resistance to blood flow in the liver's capillaries—the hepatic sinusoids[9]:83—and consequently portal hypertension, as well as impairment in other aspects of liver function.[6][10]
HepatitisB vaccine can prevent hepatitisB and the development of cirrhosis from it, but no vaccination against hepatitisC is available.[1] No specific treatment for cirrhosis is known, but many of the underlying causes may be treated by medications that may slow or prevent worsening of the condition.[3] HepatitisB and C may be treatable with antiviral medications.[1] Avoiding alcohol is recommended in all cases.[1] Autoimmune hepatitis may be treated with steroid medications.[1]Ursodiol may be useful if the disease is due to blockage of the bile duct.[1] Other medications may be useful for complications such as abdominal or leg swelling, hepatic encephalopathy, and dilated esophageal veins.[1] If cirrhosis leads to liver failure, a liver transplant may be an option.[21] Biannual screening for liver cancer using abdominal ultrasound, possibly with additional blood tests, is recommended[22][23] due to the high risk of hepatocellular carcinoma arising from dysplastic nodules.[24]
Cirrhosis affected about 2.8million people and resulted in 1.3million deaths in 2015.[4][5] Of these deaths, alcohol caused 348,000 (27%), hepatitisC caused 326,000 (25%), and hepatitisB caused 371,000 (28%).[5] In the United States, more men die of cirrhosis than women.[1] The first known description of the condition is by Hippocrates in the fifth century BCE.[25] The term "cirrhosis" was derived in 1819 from the Greek word "kirrhos", which describes the yellowish color of a diseased liver.[26]
Signs and symptoms
Person with cirrhosis and associated pain in the right upper region of the abdomen
Cirrhosis can take quite a long time to develop, and symptoms may be slow to emerge.[13] Some early symptoms include tiredness, weakness, loss of appetite, weight loss, and nausea.[13] Early signs may also include redness on the palms known as palmar erythema.[11] People may also feel discomfort in the right upper abdomen around the liver.[13]
As cirrhosis progresses, symptoms may include neurological changes affecting both the peripheral and central nervous systems, disrupting the neurotransmission within the brain and causing neuromuscular fatigue.[13][27] This can consist of cognitive impairments, confusion, memory loss, sleep disorders, and personality changes.[13] Steatorrhea or presence of undigested fats in stool is also a symptom of cirrhosis.[28]
Worsening cirrhosis can cause a build-up of fluid in different parts of the body, such as the legs (edema) and abdomen (ascites).[13] Other signs of advancing disease include itchy skin, bruising easily, dark urine, and yellowing of the skin.[13]
These features are a direct consequence of liver cells not functioning:
Spider angiomata or spider nevi happen when there is dilatation of vasculature beneath the skin surface.[29] There is a central, red spot with reddish extensions that radiate outward. This creates a visual effect that resembles a spider. It occurs in about one-third of cases.[29] The likely cause is an increase in estrogen.[29] Cirrhosis causes a rise in estrogen due to increased conversion of androgens into estrogen.[30]
Palmar erythema, a reddening of the palm below the thumb and little finger, is seen in about 23% of cirrhosis cases, and results from increased circulating estrogen levels.[31]
Gynecomastia, or the increase of breast size in men, is caused by increased estradiol (a potent type of estrogen).[32] This can occur in up to two-thirds of cases.[33]
Liver size can be enlarged, normal, or shrunken in people with cirrhosis.[36] As the disease progresses, the liver will typically shrink due to the result of scarring.[37]
Liver cirrhosis makes it hard for blood to flow in the portal venous system.[39] This resistance creates a backup of blood and increases pressure.[39] This results in portal hypertension. Effects of portal hypertension include:
Caput medusae are dilated paraumbilical collateral veins due to portal hypertension.[39] Blood from the portal venous system may be forced through the paraumbilical veins and ultimately to the abdominal wall veins. Caput Medusae The created pattern resembles the head of Medusa, hence the name.[9]
Hepatic encephalopathy (HE) occurs when ammonia and related substances build up in the blood.[45] This build-up affects brain function when they are not cleared from the blood by the liver. Symptoms can include unresponsiveness, forgetfulness, trouble concentrating, changes in sleep habits, or psychosis. One classic physical examination finding is asterixis.[33] This is the asynchronous flapping of outstretched, dorsiflexed hands.[33]Fetor hepaticus is a musty breath odor resulting from increased dimethyl sulfide and is a feature of HE.[46]
Increased sensitivity to medication can be caused by decreased metabolism of the active compounds.[47]
Cirrhosis has many possible causes, and more than one cause may be present. History taking is of importance in trying to determine the most likely cause.[2] Globally, 57% of cirrhosis is attributable to either hepatitisB (30%) or hepatitisC (27%).[48][49]Alcohol use disorder is another major cause, accounting for about 20–40% of the cases.[49][33]
Alcoholic liver disease (ALD, or alcoholic cirrhosis) develops in 10–20% of individuals who drink heavily for a decade or more.[50] Alcohol seems to injure the liver by blocking the normal metabolism of protein, fats, and carbohydrates.[51] This injury happens through the formation of acetaldehyde from alcohol. Acetaldehyde is reactive and leads to the accumulation of other reactive products in the liver.[33] People with ALD may also have concurrent alcoholic hepatitis. Associated symptoms are fever, hepatomegaly, jaundice, and anorexia.[51]AST and ALT blood levels are both elevated, but at less than 300 IU/liter, with an AST:ALT ratio > 2.0, a value rarely seen in other liver diseases.[52] In the United States, 40% of cirrhosis-related deaths are due to alcohol.[33]
In non-alcoholic fatty liver disease (NAFLD), fat builds up in the liver and eventually causes scar tissue.[53] This type of disorder can be caused by obesity, diabetes, malnutrition, coronary artery disease, and steroids.[53][54] Though similar in signs to alcoholic liver disease, no history of notable alcohol use is found. Blood tests and medical imaging are used to diagnose NAFLD and NASH, and sometimes a liver biopsy is needed.[40]
Chronic hepatitis C, an infection with the hepatitis C virus, causes inflammation of the liver and a variable grade of damage to the organ.[45] Over several decades, this inflammation and damage can lead to cirrhosis. Among people with chronic hepatitisC, 20–30% develop cirrhosis.[45][33] Cirrhosis caused by hepatitisC and alcoholic liver disease are the most common reasons for liver transplant.[33]
Chronic hepatitis B causes liver inflammation and injury that, over several decades, can lead to cirrhosis.[45] HepatitisD is dependent on the presence of hepatitisB and accelerates cirrhosis in co-infection.[45]
Autoimmune hepatitis is caused by an attack of the liver by lymphocytes. This causes inflammation and eventually scarring as well as cirrhosis. Findings include elevations in serum globulins, especially gamma globulins.[33]
The liver plays a vital role in many metabolic processes in the body, including protein synthesis, detoxification, nutrient storage (such as glycogen), platelet production, and clearance of bilirubin. With progressive liver damage, hepatocyte death, and replacement of functional liver tissue with fibrosis in cirrhosis, these processes are disrupted. This leads to many of the metabolic derangements and symptoms seen in cirrhosis.[58]
Cirrhosis is often preceded by hepatitis and fatty liver (steatosis), independent of the cause. If the cause is removed at this stage, the changes are fully reversible.[citation needed]
The pathological hallmark of cirrhosis is the development of scar tissue that replaces normal tissue, which is normally organized into lobules. This scar tissue blocks the portal flow of blood through the organ, raising the blood pressure.[58] This manifests as portal hypertension in which the pressure gradient between the portal circulation as compared to the systemic circulation is elevated. This portal hypertension leads to decreased sinusoidal flow from liver cells to nearby sinusoids in the liver, and increased lymph production with extravasation of lymph to the extracellular space, causing ascites.[58] This also causes reduced cardiac return and central blood volume, which activates the renin-angiotensin system (RAAS), which causes kidneys to reabsorb sodium and water, causing water retention and further ascites. Activation of the RAAS also causes kidney vasoconstriction and may cause kidney injury.[58]
Research has shown the pivotal role of the stellate cell, which normally stores vitamin A, in the development of cirrhosis. Damage to the liver tissue from inflammation leads to the activation of stellate cells, which increases fibrosis through the production of myofibroblasts, and obstructs hepatic blood flow.[59] In addition, stellate cells secrete TGF beta 1, which leads to a fibrotic response and proliferation of connective tissue. TGF-β1 has been implicated in the process of activating hepatic stellate cells (HSCs), with the magnitude of fibrosis being in proportion to the increase in TGF-β levels. ACTA2 is associated with the TGF-β pathway that enhances contractile properties of HSCs, leading to fibrosis.[60] Furthermore, HSCs secrete TIMP1 and TIMP2, naturally occurring inhibitors of matrix metalloproteinases (MMPs), which prevent MMPs from breaking down the fibrotic material in the extracellular matrix.[61][62]
As this cascade of processes continues, fibrous tissue bands (septa) separate hepatocyte nodules, which eventually replace the entire liver architecture, leading to decreased blood flow throughout. The spleen becomes congested, and enlarged, resulting in its retention of platelets, which are needed for normal blood clotting. Portal hypertension is responsible for the most severe complications of cirrhosis.[citation needed]
The diagnosis of cirrhosis in an individual is based on multiple factors.[33] Cirrhosis may be suspected from laboratory findings, physical exam, and the person's medical history. Imaging is generally obtained to evaluate the liver.[33] A liver biopsy will confirm the diagnosis; however, is generally not required.[45]
Imaging
Ultrasound is routinely used in the evaluation of cirrhosis.[45] It may show a small and shrunken liver in advanced disease. On ultrasound, there is increased echogenicity with irregular appearing areas.[63] Other suggestive findings are an enlarged caudate lobe, liver surface nodularity[64] widening of the fissures and enlargement of the spleen.[65] An enlarged spleen, which normally measures less than 11–12cm (4.3–4.7in) in adults, may suggest underlying portal hypertension.[66] Ultrasound may also screen for hepatocellular carcinoma and portal hypertension.[45] This is done by assessing flow in the hepatic vein.[67] An increased portal vein pulsatility may be seen. However, this may be a sign of elevated right atrial pressure.[68] Portal vein pulsatility is usually measured by a pulsatility index (PI).[67] A number above a certain value indicates cirrhosis (see table below).
Other scans include CT of the abdomen and MRI.[45] A CT scan is non-invasive and may be helpful in the diagnosis.[45] Compared to the ultrasound, CT scans tend to be more expensive. MRI provides excellent evaluation; however, it is expensive.[45]
Rarely are diseases of the bile ducts, such as primary sclerosing cholangitis, causes of cirrhosis.[45] Imaging of the bile ducts, such as ERCP or MRCP (MRI of biliary tract and pancreas) may aid in the diagnosis.[45]
Lab findings
The best predictors of cirrhosis are ascites, platelet count <160,000/mm3, spider angiomata, and a Bonacini cirrhosis discriminant score greater than 7 (as the sum of scores for platelet count, ALT/AST ratio and INR as per table).[76]
Thrombocytopenia, typically multifactorial, is due to alcoholic marrow suppression, sepsis, lack of folate, platelet sequestering in the spleen, and decreased thrombopoietin.[52] However, this rarely results in a platelet count <50,000/mL.[78]
Aminotransferases AST and ALT are moderately elevated, with AST > ALT. However, normal aminotransferase levels do not preclude cirrhosis.[52]
Vasoactive intestinal peptide is increased as blood is shunted into the intestinal system because of portal hypertension.
Vasodilators are increased (such as nitric oxide and carbon monoxide) reducing afterload with compensatory increase in cardiac output, mixed venous oxygen saturation.[79]
Renin is increased (as well as sodium retention in kidneys) secondary to a fall in systemic vascular resistance.[80]
FibroTest is a biomarker for fibrosis that may be used instead of a biopsy.[81]
Other laboratory studies performed in newly diagnosed cirrhosis may include:
Immunoglobulin levels (IgG, IgM, IgA) – these immunoglobulins are nonspecific, but may help in distinguishing various causes.
IgG level is elevated in chronic hepatitis, alcoholic hepatitis, and autoimmune hepatitis. It is a slow and sustained increase is seen in viral hepatitis.
IgM significantly increased in primary biliary cirrhosis and moderately increased in viral hepatitis and cirrhosis.
IgA is increased in alcoholic cirrhosis and primary biliary cirrhosis.[citation needed]
Cholesterol and glucose
Alpha 1-antitrypsin
Markers of inflammation and immune cell activation are typically elevated in cirrhotic patients, especially in the decompensated disease stage:
The link between gut microbiota constitution and liver health (Particularly in Cirrhosis) has been well described,[89] however specific biomarkers for prediction of Cirrhosis still requires further research. A 2014 study identified 15 microbial biomarkers from the gut microbiota.[90] These could potentially be used to discriminate patients with liver cirrhosis from healthy individuals.
The gold standard for diagnosis of cirrhosis is a liver biopsy. This is usually carried out as a fine-needle approach, through the skin (percutaneous), or internal jugular vein (transjugular).[91] Endoscopic ultrasound-guided liver biopsy (EUS), using the percutaneous or transjugular route, has become a good alternative to use.[92][91] EUS can target liver areas that are widely separated,[93] and can deliver bi-lobar biopsies.[92] A biopsy is not necessary if the clinical, laboratory, and radiologic data suggest cirrhosis. Furthermore, a small but significant risk of complications is associated with liver biopsy, and cirrhosis itself predisposes to complications caused by liver biopsy.[94]
Once the biopsy is obtained, a pathologist will study the sample. Cirrhosis is defined by its features on microscopy: (1) the presence of regenerating nodules of hepatocytes and (2) the presence of fibrosis, or the deposition of connective tissue between these nodules. The pattern of fibrosis seen can depend on the underlying insult that led to cirrhosis. Fibrosis can also proliferate even if the underlying process that caused it has resolved or ceased. The fibrosis in cirrhosis can lead to destruction of other normal tissues in the liver, including the sinusoids, the space of Disse, and other vascular structures, which leads to altered resistance to blood flow in the liver, and portal hypertension.[95]
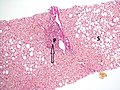
No fibrosis, but mild zone 3 steatosis, in which collagen fibres (pink–red, arrow) are confined to portal tracts (P) (Van Gieson's stain)[96]
Histopathology of steatohepatitis with mild fibrosis in the form of fibrous expansion (Van Gieson's stain)[96]
Histopathology of steatohepatitis with moderate fibrosis, with thin fibrous bridges (Van Gieson's stain)[96]
Histopathology of steatohepatitis with established cirrhosis, with thick bands of fibrosis (Van Gieson's stain)[96]
Trichrome stain, showing cirrhosis as a nodular texture surrounded by fibrosis (wherein collagen is stained blue)
As cirrhosis can be caused by many different entities that injure the liver in different ways, cause-specific abnormalities may be seen. For example, in chronic hepatitisB, there is infiltration of the liver parenchyma with lymphocytes.[95] In congestive hepatopathy there are erythrocytes and a greater amount of fibrosis in the tissue surrounding the hepatic veins.[97] In primary biliary cholangitis, there is fibrosis around the bile duct, the presence of granulomas and pooling of bile.[98] Lastly in alcoholic cirrhosis, there is infiltration of the liver with neutrophils.[95]
Macroscopically, the liver is initially enlarged, but with the progression of the disease, it becomes smaller. Its surface is irregular, the consistency is firm, and if associated with steatosis, the color is yellow. Depending on the size of the nodules, there are three macroscopic types: micronodular, macronodular, and mixed cirrhosis. In the micronodular form (Laennec's cirrhosis or portal cirrhosis), regenerating nodules are under 3mm. In macronodular cirrhosis (post-necrotic cirrhosis), the nodules are larger than 3mm. Mixed cirrhosis consists of nodules of different sizes.[99]
Micronodular cirrhosis, with diffuse areas of pallor
Pale macronodules of cirrhosis
Cirrhosis leading to hepatocellular carcinoma
Grading
The severity of cirrhosis is commonly classified with the Child–Pugh score (also known as the Child–Pugh–Turcotte score).[100] This system was devised in 1964 by Child and Turcotte, and modified in 1973 by Pugh and others.[101] It was first established to determine who would benefit from elective surgery for portal decompression.[100] This scoring system uses multiple lab values including bilirubin, albumin, and INR.[102] The presence of ascites and severity of encephalopathy is also included in the scoring.[102] The classification system includes class A, B, or C.[102] Class A has a favorable prognosis while class C is at high risk of death.
Child-Pugh Score in Relation to Liver Function, Prognosis and Post-op Mortality[102][100]
Child-Pugh Class
Points
Liver Function
Prognosis
Abdominal surgery post-operative mortality
Child-Pugh Class A
5–6 points
Good liver function
15–20 years
10%
Child-Pugh Class B
7–9 points
Moderately impaired liver function
30%
Child-Pugh Class C
10–15 points
Advanced liver dysfunction
1–3 years
82%
The Child-Pugh score is a validated predictor of mortality after a major surgery.[100] For example, Child class A patients have a 10% mortality rate and Child class B patients have a 30% mortality rate while Child class C patients have a 70–80% mortality rate after abdominal surgery.[100] Elective surgery is usually reserved for those in Child class A patients. There is an increased risk for Child class B individuals, and they may require medical optimization. Overall, it is not recommended for Child class C patients to undergo elective surgery.[100]
In the past, the Child-Pugh classification was used to determine people who were candidates for a liver transplant.[100] Child-Pugh class B is usually an indication for evaluation for transplant.[102] However, there were many issues when applying this score to liver transplant eligibility.[100] Thus, the MELD score was created.
The Model for End-Stage Liver Disease (MELD) score was later developed and approved in 2002.[103] It was approved by the United Network for Organ Sharing (UNOS) as a way to determine the allocation of liver transplants to awaiting people in the United States.[104] It is also used as a validated survival predictor of cirrhosis, alcoholic hepatitis, acute liver failure, and acute hepatitis.[105] The variables included bilirubin, INR, creatinine, and dialysis frequency.[105] In 2016, sodium was added to the variables and the score is often referred to as MELD-Na.[106]
MELD-Plus is a further risk score to assess the severity of chronic liver disease. It was developed in 2017 as a result of a collaboration between Massachusetts General Hospital and IBM.[107] Nine variables were identified as effective predictors for 90-day mortality after a discharge from a cirrhosis-related hospital admission.[107] The variables include all Model for End-Stage Liver Disease (MELD)'s components, as well as sodium, albumin, total cholesterol, white blood cell count, age, and length of stay.[107]
Key prevention strategies for cirrhosis are population-wide interventions to reduce alcohol intake (through pricing strategies, public health campaigns, and personal counseling), programs to reduce the transmission of viral hepatitis, and screening of relatives of people with hereditary liver diseases.[109]
Little is known about factors affecting cirrhosis risk and progression. However, many studies have provided increasing evidence for the protective effects of coffee consumption against the progression of liver disease. These effects are more noticeable in liver disease that is associated with alcohol use disorder. Coffee has antioxidant and antifibrotic effects. Caffeine may not be the important component; polyphenols may be more important. Drinking two or more cups of coffee a day is associated with improvements in the liver enzymesALT, AST, and GGT. Even in those with liver disease, coffee consumption can lower fibrosis and cirrhosis.[110]
Treatment
Generally, liver damage from cirrhosis cannot be reversed, but treatment can stop or delay further progression and reduce complications. A healthy diet is encouraged, as cirrhosis may be an energy-consuming process. A recommended diet consists of a high-protein, high-fiber diet plus supplementation with branched-chain amino acids.[111] Close follow-up is often necessary. Antibiotics are prescribed for infections, and various medications can help with itching. Laxatives, such as lactulose, decrease the risk of constipation. Carvedilol increases survival benefit for people with cirrhosis and portal hypertension.[112] Diuretics in combination with a low-salt diet reduce fluid in the body, which helps reduce oedema.[113]
Alcoholic cirrhosis caused by alcohol use disorder is treated by abstaining from alcohol. Treatment for hepatitis-related cirrhosis involves medications used to treat the different types of hepatitis, such as interferon for viral hepatitis and corticosteroids for autoimmune hepatitis.[citation needed]
As of 2021, there are recent studies studying drugs to prevent cirrhosis caused by non-alcoholic fatty liver disease (NAFLD or NASH). The drug semaglutide was shown to provide greater NASH resolution versus placebo. No improvement in fibrosis was observed.[114] A combination of cilofexor/firsocostat was studied in people with bridging fibrosis and cirrhosis. It was observed to have led to improvements in NASH activity with a potential antifibrotic effect.[115] Lanifibranor is also shown to prevent worsening fibrosis.[116]
Preventing further liver damage
Regardless of the underlying cause of cirrhosis, consumption of alcohol and other potentially damaging substances is discouraged. There is no evidence that supports the avoidance or dose reduction of paracetamol in people with compensated cirrhosis; it is thus considered a safe analgesic for said individuals.[117]
Vaccination against hepatitisA and hepatitisB is recommended early in the course of illness due to a decline in effectiveness of the vaccines with decompensation.[118]
Treating the cause of cirrhosis prevents further damage; for example, giving oral antivirals such as entecavir and tenofovir where cirrhosis is due to hepatitisB prevents progression of cirrhosis. Similarly, control of weight and diabetes prevents deterioration in cirrhosis due to non-alcoholic fatty liver disease.[119]
People with cirrhosis or liver damage are often advised to avoid drugs that could further harm the liver.[120] These include several drugs such as anti-depressants, certain antibiotics, and NSAIDs (like ibuprofen).[120] These agents are hepatotoxic as they are metabolized by the liver. If a medication that harms the liver is still recommended by a doctor, the dosage can be adjusted to aim for minimal stress on the liver.[citation needed]
Lifestyle
According to a 2018 systematic review based on studies that implemented 8 to 14 week-long exercise programs, there is currently insufficient scientific evidence regarding either the beneficial or harmful effects of physical exercise in people with cirrhosis on all-cause mortality, morbidity (including both serious and non-serious adverse events), health-related quality of life, exercise capacity and anthropomorphic measures.[121] These conclusions were based on low to very low quality research, which imposes the need to develop further research with higher quality, especially to evaluate its effects on clinical outcomes.[citation needed]
If complications cannot be controlled or when the liver ceases functioning, liver transplantation is necessary. Survival from liver transplantation has been improving over the 1990s, and the five-year survival rate is now around 80%. The survival rate depends largely on the severity of the disease and other medical risk factors in the recipient.[122] In the United States, the MELD score is used to prioritize patients for transplantation.[123] Transplantation necessitates the use of immune suppressants (ciclosporin or tacrolimus).
People with decompensated cirrhosis generally require admission to a hospital, with close monitoring of the fluid balance, mental status, and emphasis on adequate nutrition and medical treatment – often with diuretics, antibiotics, laxatives or enemas, thiamine and occasionally steroids, acetylcysteine and pentoxifylline.[124] Administration of saline is avoided, as it would add to the already high total body sodium content that typically occurs in cirrhosis. Life expectancy without a liver transplant is low, at most three years.
Palliative care
Palliative care is specialized medical care that focuses on providing patients with relief from the symptoms, pain, and stress of a serious illness, such as cirrhosis. The goal of palliative care is to improve quality of life for both the patient and the patient's family, and it is appropriate at any stage and for any type of cirrhosis.[125]
Especially in the later stages, people with cirrhosis experience significant symptoms such as abdominal swelling, itching, leg edema, and chronic abdominal pain, which would be amenable to treatment through palliative care.[126] Because the disease is not curable without a transplant, palliative care can also help with discussions regarding the person's wishes concerning health care power of attorney, do not resuscitate decisions and life support, and potentially hospice.[126] Despite proven benefit, people with cirrhosis are rarely referred to palliative care.[127]
Immune system
Cirrhosis is known to cause immune dysfunction in numerous ways. It impedes the immune system from working normally.[128]
Bleeding and blood clot risk
Cirrhosis can increase the risk of bleeding. The liver produces various proteins in the coagulation cascade (coagulation factors II, VII, IX, X, V, and VI). When damaged, the liver is impaired in its production of these proteins.[129] This will ultimately increase bleeding as clotting factors are diminished. Clotting function is estimated by lab values, mainly platelet count, prothrombin time (PT), and international normalized ratio (INR).
The AGA does not recommend extensive pre-procedural testing, including repeated measurements of PT/INR or platelet count, before patients with stable cirrhosis undergo common gastrointestinal procedures. Nor do they suggest the routine use of blood products, such as platelets, for bleeding prevention.[129] Cirrhosis is stable when there are no changes in baseline abnormalities of coagulation lab values.
For patients with stable cirrhosis and low platelet count undergoing common low-risk procedures, the AGA does not recommend the routine use of thrombopoietin receptor agonists for bleeding prevention.[129]
In hospitalized patients who meet standard guidelines for clot prevention, the AGA suggests standard prevention.[129]
The AGA does not recommend routine screening for portal vein thrombosis. If there is a portal vein thrombosis, the AGA suggests treatment by anticoagulation.[129]
In the case of cirrhosis with atrial fibrillation, the AGA recommends using anticoagulation over no anticoagulation.[129]
Complications
Ascites
Salt restriction is often necessary, as cirrhosis leads to the accumulation of salt (sodium retention). Diuretics may be necessary to suppress ascites. Diuretic options for inpatient treatment include aldosterone antagonists (spironolactone) and loop diuretics. Aldosterone antagonists are preferred for people who can take oral medications and do not need an urgent volume reduction. Loop diuretics can be added as additional therapy.[130]
Where salt restriction and the use of diuretics are ineffective, then paracentesis may be the preferred option.[131] This procedure requires the insertion of a plastic tube into the peritoneal cavity. Human serum albumin solution is usually given to prevent complications from the rapid volume reduction. In addition to being more rapid than diuretics, 4–5 liters of paracentesis is more successful in comparison to diuretic therapy.[130]
Esophageal and gastric variceal bleeding
For portal hypertension, nonselective beta blockers, such as propranolol or nadolol, are commonly used to lower blood pressure over the portal system. In severe complications from portal hypertension, transjugular intrahepatic portosystemic shunting (TIPS) is occasionally indicated to relieve pressure on the portal vein. As this shunting can worsen hepatic encephalopathy, it is reserved for those patients at low risk of encephalopathy. TIPS is generally regarded only as a bridge to liver transplantation[132] or as a palliative measure.[citation needed] Balloon-occluded retrograde transvenous obliteration can be used to treat gastric variceal bleeding.[133]
Hepatic encephalopathy is a potential complication of cirrhosis.[33] It may lead to functional neurological impairment ranging from mild confusion to coma.[33] Hepatic encephalopathy is primarily caused by the accumulation of ammonia in the blood, which causes neurotoxicity when crossing the blood-brain barrier. Ammonia is normally metabolized by the liver; as cirrhosis causes both decreased liver function and increased portosystemic shunting (allowing blood to bypass the liver), systemic ammonia levels gradually rise and lead to encephalopathy.[137]
Most pharmaceutical approaches to treating hepatic encephalopathy focus on reducing ammonia levels.[138] Per 2014 guidelines,[139] the first-line treatment involves the use of lactulose, a non-absorbable disaccharide which decreases the pH level of the colon when it is metabolized by intestinal bacteria. The lower colonic pH causes increased conversion of ammonia into ammonium, which is then excreted from the body.[140]Rifaximin, an antibiotic that inhibits the function of ammonia-producing bacteria in the gastrointestinal tract,[141] is recommended for use in combination with lactulose as prophylaxis against recurrent episodes of hepatic encephalopathy.[139][142][143]
In addition to pharmacotherapy, providing proper hydration and nutritional support is also essential.[138] Appropriate quantities of protein uptake are encouraged.[144] Several factors may precipitate hepatic encephalopathy, which include alcohol use, excess protein, gastrointestinal bleeding, infection, constipation, and vomiting/diarrhea.[138] Drugs such as benzodiazepines, diuretics, or narcotics can also precipitate encephalopathic events.[138] A low protein diet is recommended with gastrointestinal bleeding.[144]
The severity of hepatic encephalopathy is determined by assessing the patient's mental status. This is generally a subjective assessment, although several attempts at creating criteria to help standardize this assessment have been published. One example is the West Haven criteria, reproduced below.
People with cirrhosis have a 40% lifetime risk of developing hepatic encephalopathy.[58] The median survival after the development of hepatic encephalopathy is 0.9 years.[58] Mild hepatic encephalopathy (also known as covert hepatic encephalopathy), in which symptoms are more subtle, such as impairments in executive function, poor sleep or balance impairment is also associated with a higher risk of hospitalization and death (18% in those with covert hepatic encephalopathy vs 3% in those with cirrhosis and no HE).[58]
Hepatorenal syndrome
Hepatorenal syndrome is a serious complication of end-stage cirrhosis when kidney damage is also involved.[146] The annual risk of developing hepatorenal syndrome in those with cirrhosis is 8% and once the syndrome develops the median survival is 2 weeks.[58]
Cirrhosis can cause immune system dysfunction, leading to infection. Signs and symptoms of infection may be nonspecific and are more difficult to recognize (for example, worsening encephalopathy but no fever).[148] Moreover, infections in cirrhosis are major triggers for other complications (ascites, variceal bleeding, hepatic encephalopathy, organ failures, death).[148][86][88]
Those with cirrhosis are at increased risk of infections as well as increased mortality from infections. This is due to a combination of factors, including cirrhosis-associated immune dysfunction, reduced gut barrier function, reduced bile flow, and changes in the gut microbiota, with an increase in pathobionts (native bacteria that, under certain conditions, may cause infection).[128]
Cirrhosis associated immune dysfunction is caused by reduced complement component synthesis in the liver including C3, C4 and reduced total complement activity (CH50).[128] The complement system is a part of the innate immune system and assists immune cells and antibodies in destroying pathogens. The liver produces complement factors, but this may be reduced in cirrhosis, raising the risk of infections. Acute phase proteins (which help mount an immune response) and soluble pattern recognition receptors (which help immune cells to identify pathogens) are also reduced in those with cirrhosis, leading to further immune dysfunction.[128] Cirrhosis is also associated with reduced Kupfer cell function, further increasing the risk for infections. Kupfer cells are resident macrophages in the liver, which help to destroy pathogens.[128]
Extrinsic factors may also increase the risk of infection in those with cirrhosis, including proton pump inhibitor use, alcohol use, frailty, antibiotic overuse, and hospitalizations or invasive procedures (which increase the risk of bacterial translocation to other areas of the body).[128]
Infections that are common in those in the hospital with cirrhosis include spontaneous bacterial peritonitis (with a prevalence of 27% among hospitalized patients), urinary tract infections (22-29%), pneumonia (19%), spontaneous bacteremia (8-13%), skin and soft tissue infections (8-12%) and C. difficile colitis (2.4-4%).[128][149] It is estimated that 3.5% of people with cirrhosis and ascites may have asymptomatic spontaneous bacterial peritonitis.[150]
The mortality rate for infections in those with cirrhosis is higher than that of the general population. In those with cirrhosis and severe infections with sepsis, the mortality rate is greater than 50%, and in those with septic shock, the mortality rate is 65%.[128]
Each year, approximately one million deaths are due to complications of cirrhosis, making cirrhosis the 11th most common cause of death globally.[154] Cirrhosis and chronic liver disease were the tenth leading cause of death for men and the twelfth for women in the United States in 2001, killing about 27,000 people each year.[155]
The cause of cirrhosis can vary; alcohol and non-alcoholic fatty liver disease are main causes in western and industrialized countries, whereas viral hepatitis is the predominant cause in low and middle-income countries.[154] Cirrhosis is more common in men than in women.[156] The cost of cirrhosis in terms of human suffering, hospital costs, and lost productivity is high.
Globally, age-standardized disability-adjusted life year (DALY) rates have decreased from 1990 to 2017, with the values going from 656.4 years per 100,000 people to 510.7 years per 100,000 people.[157] In males DALY rates have decreased from 903.1 years per 100,000 population in 1990, to 719.3 years per 100,000 population in 2017; in females the DALY rates have decreased from 415.5 years per 100,000 population in 1990, to 307.6 years per 100,000 population in 2017.[157] However, globally the total number of DALYs has increased by 10.9million from 1990 to 2017, reaching the value of 41.4million DALYs.[157]
Etymology
The word "cirrhosis" is a neologism derived from Greek: κίρρωσις; kirrhosκιρρός, meaning "yellowish, tawny" (the orange yellow colour of the diseased liver) and the suffix -osis, i.e., "condition" in medical terminology.[158][159][160] While the clinical entity was known before, René Laennec gave it this name in an 1819 paper.[26]
12345678910111213141516"Cirrhosis". National Institute of Diabetes and Digestive and Kidney Diseases. April 23, 2014. Archived from the original on 9 June 2015. Retrieved 19 May 2015.
↑Sharma B, John S (31 October 2022). "Hepatic Cirrhosis". StatPearls [Internet]. Treasure Island, Florida: StatPearls Publishing. PMID29494026. Bookshelf ID NBK482419. Retrieved 16 July 2024– via National Library of Medicine.
123Bansal MB, Friedman SL (8 June 2018). "Chapter 6: Hepatic Fibrinogenesis". In Dooley JS, Lok AS, Garcia-Tsao G, Pinzani M (eds.). Sherlock's diseases of the liver and biliary system (13thed.). Hoboken, New Jersey: Wiley Blackwell. pp.82–92. ISBN978-1-119-23756-3. OCLC1019837000.
↑McCormick PA, Jalan R (8 June 2018). "Chapter 8: Hepatic Cirrhosis". In Dooley JS, Lok AS, Garcia-Tsao G, Pinzani M (eds.). Sherlock's diseases of the liver and biliary system (13thed.). Hoboken, New Jersey: Wiley Blackwell. pp.107–126. ISBN978-1-119-23756-3. OCLC1019837000.
↑Ilić G, Karadžić R, Kostić-Banović L, Stojanović J, Antović A (February 2010). "Ultrastructural Changes In The Liver Of Intravenous Heroin Addiction". Bosnian Journal of Basic Medical Sciences. Vol.10, no.1. Journal of the Association of Basic Medical Sciences. pp.36–43. PMC5596609.
↑Feingold KR, Anawalt B, Boyce A, Chrousos G, de Herder WW, Dhatariya K, etal. (2000). "Gynecomastia: Etiology, Diagnosis, and Treatment". In Feingold KR, Anawalt B, Boyce A, Chrousos G (eds.). Endotext. South Dartmouth (MA): MDText.com, Inc. PMID25905330. Retrieved 2022-03-16.
123456789101112131415161718192021Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. (2012). Harrison's principles of internal medicine (18thed.). New York: McGraw-Hill. pp.Chapter 308. Cirrhosis and Its Complications. ISBN978-0-07-174889-6.
↑Kim SM, Yalamanchi S, Dobs AS (2017). "Male Hypogonadism and Liver Disease". In Winters SJ, Huhtaniemi IT (eds.). Male Hypogonadism. Cham: Springer International Publishing. pp.219–234. doi:10.1007/978-3-319-53298-1_11. ISBN978-3-319-53296-7.
↑Alabama Jennifer A. Gentile, PharmD Candidate 2021 Logan B. Boone, PharmD Candidate 2021 Samford University McWhorter School of Pharmacy Birmingham, Alabama Jeffrey A. Kyle, PharmD, BCPS Professor of Pharmacy Practice Samford University McWhorter School of Pharmacy Birmingham, Alabama Langley R. Kyle, PharmD Clinical Pharmacy Specialist RxBenefits Birmingham. "Drug Considerations for Medication Therapy in Cirrhosis". www.uspharmacist.com. Retrieved 2024-11-08.{{cite web}}: CS1 maint: multiple names: authors list (link) CS1 maint: numeric names: authors list (link)
12Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP (October 2006). "The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide". Journal of Hepatology. 45 (4): 529–538. doi:10.1016/j.jhep.2006.05.013. PMID16879891.
123Friedman LS (2014). Current medical diagnosis and treatment 2014. [S.l.]: Mcgraw-Hill. pp.Chapter 16. Liver, Biliary Tract, & Pancreas Disorders. ISBN978-0-07-180633-6.
12345Machado MV, Diehl AM (2018). "Pathogenesis of Nonalcoholic Fatty Liver Disease". In Sanyal AJ, Boyer TD, Terrault NA, Lindor KD (eds.). Zakim and Boyer's Hepatology. pp.369–390. doi:10.1016/c2013-0-19055-1. ISBN978-0-323-37591-7.
↑Hammer GD, McPhee SJ, eds. (2010). Pathophysiology of disease: an introduction to clinical medicine (6thed.). New York: McGraw-Hill Medical. pp.Chapter 14: Liver Disease. Cirrhosis. ISBN978-0-07-162167-0.
12Dietrich CF (2009). "Ultrasonography". In Dancygier H (ed.). Clinical Hepatology: Principles and Practice of Hepatobiliary Diseases. Vol.1. Springer Science & Business Media. p.367. ISBN978-3-540-93842-2. Archived from the original on 2018-11-30.
12Maddrey WC, Schiff ER, Sorrell MF, eds. (1999). Schiff's diseases of the liver (11thed.). Chichester, West Sussex, UK: John Wiley & Sons. pp.Evaluation of the Liver A: Laboratory Test. ISBN978-0-470-65468-2.
↑Slater JS, Esherick DS, Clark ED (2012-12-18). Current practice guidelines in primary care 2013. New York: McGraw-Hill Medical. pp.Chapter 3: Disease Management. ISBN978-0-07-179750-4.
↑Van Thiel DH, Gavaler JS, Schade RR (February 1985). "Liver disease and the hypothalamic pituitary gonadal axis". Seminars in Liver Disease. 5 (1): 35–45. doi:10.1055/s-2008-1041756. PMID3983651. S2CID35436861.
↑Halfon P, Munteanu M, Poynard T (September 2008). "FibroTest-ActiTest as a non-invasive marker of liver fibrosis". Gastroenterologie Clinique et Biologique. 32 (6 Suppl 1): 22–39. doi:10.1016/S0399-8320(08)73991-5. PMID18973844.
↑Laursen TL, Rødgaard-Hansen S, Møller HJ, Mortensen C, Karlsen S, Nielsen DT, etal. (April 2017). "The soluble mannose receptor is released from the liver in cirrhotic patients, but is not associated with bacterial translocation". Liver International. 37 (4): 569–575. doi:10.1111/liv.13262. PMID27706896. S2CID46856702.
↑Grant A, Neuberger J (October 1999). "Guidelines on the use of liver biopsy in clinical practice. British Society of Gastroenterology". Gut. 45 (Suppl 4): IV1–IV11. doi:10.1136/gut.45.2008.iv1. PMC1766696. PMID10485854. Archived from the original on 2007-06-30. The main cause of mortality after percutaneous liver biopsy is intraperitoneal haemorrhage as shown in a retrospective Italian study of 68,000 percutaneous liver biopsies, in which all six patients who died did so from intraperitoneal haemorrhage. Three of these patients had had a laparotomy, and all had either cirrhosis or malignant disease, both of which are risk factors for bleeding.
123Brenner D, Rippe RA (2003). "Pathogenesis of Hepatic Fibrosis". In Yamada (ed.). Textbook of Gastroenterology. Vol.2 (4thed.). Lippincott Williams & Wilkins. ISBN978-0-7817-2861-4.
12345678Tsoris A, Marlar CA (2022). "Use Of The Child Pugh Score In Liver Disease". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID31194448. Retrieved 2022-03-23.
↑Loomba R, Noureddin M, Kowdley KV, Kohli A, Sheikh A, Neff G, etal. (February 2021). "Combination Therapies Including Cilofexor and Firsocostat for Bridging Fibrosis and Cirrhosis Attributable to NASH". Hepatology. 73 (2): 625–643. doi:10.1002/hep.31622. PMID33169409. S2CID226295213.
↑Bajaj JS, Kamath PS, Reddy KR (2021). "The Evolving Challenge of Infections in Cirrhosis". The New England Journal of Medicine. 384 (24): 2317–2330. doi:10.1056/NEJMra2021808. PMID34133861.
12Sanchez W, Talwalkar JA (March 2006). "Palliative care for patients with end-stage liver disease ineligible for liver transplantation". Gastroenterology Clinics of North America. 35 (1): 201–219. doi:10.1016/j.gtc.2005.12.007. PMID16530121.
↑Poonja Z, Brisebois A, van Zanten SV, Tandon P, Meeberg G, Karvellas CJ (April 2014). "Patients with cirrhosis and denied liver transplants rarely receive adequate palliative care or appropriate management". Clinical Gastroenterology and Hepatology. 12 (4): 692–698. doi:10.1016/j.cgh.2013.08.027. PMID23978345.
12345678Bajaj JS, Kamath PS, Reddy KR (17 June 2021). "The Evolving Challenge of Infections in Cirrhosis". New England Journal of Medicine. 384 (24): 2317–2330. doi:10.1056/NEJMra2021808. PMID34133861.
↑Sellers CM, Nezami N, Schilsky ML, Kim HS (April 2019). "Transjugular intrahepatic portosystemic shunt as a bridge to liver transplant: Current state and future directions". Transplantation Reviews. 33 (2): 64–71. doi:10.1016/j.trre.2018.10.004. PMID30477811. S2CID53736623.
↑Piano S, Singh V, Caraceni P (April 2019). "Epidemiology and Effects of Bacterial Infections in Patients With Cirrhosis Worldwide". Gastroenterology. 156 (5): 1368–1380.e10. doi:10.1053/j.gastro.2018.12.005. PMID30552895.
↑Evans L, Ray Kim W, Poterucha J, Kamath P (April 2003). "Spontaneous bacterial peritonitis in asymptomatic outpatients with cirrhotic ascites". Hepatology. 37 (4): 897–901. doi:10.1053/jhep.2003.50119. PMID12668984.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.