| Pneumoperitoneum | |
|---|---|
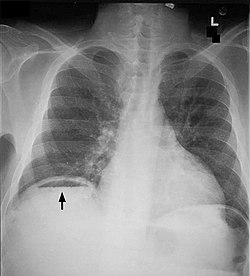 | |
| Frontal chest X-ray. The air bubble below the right hemidiaphragm (on the left of the image) is a pneumoperitoneum. | |
| Specialty | Gastroenterology |
Pneumoperitoneum is pneumatosis (abnormal presence of air or other gas) in the peritoneal cavity, a potential space within the abdominal cavity. The most common cause is a perforated abdominal organ, generally from a perforated peptic ulcer, although any part of the bowel may perforate from a benign ulcer, tumor or abdominal trauma. A perforated appendix rarely causes a pneumoperitoneum.
Contents
- Causes
- Spontaneous pneumoperitoneum
- Diagnosis
- Differential diagnosis
- Treatment
- Terminology
- See also
- References
- External links
Spontaneous pneumoperitoneum is a rare case that is not caused by an abdominal organ rupture. This is also called an idiopathic spontaneous pneumoperitoneum when the cause is not known.
In the mid-twentieth century, an "artificial" pneumoperitoneum was sometimes intentionally administered as a treatment for a hiatal hernia. This was achieved by insufflating the abdomen with carbon dioxide. The practice is currently used by surgical teams in order to aid in performing laparoscopic surgery.


