
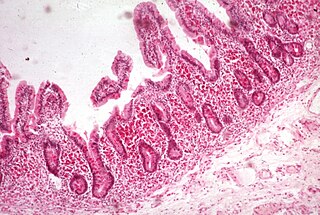
In vertebrates, the gallbladder, also known as the cholecyst, is a small hollow organ where bile is stored and concentrated before it is released into the small intestine. In humans, the pear-shaped gallbladder lies beneath the liver, although the structure and position of the gallbladder can vary significantly among animal species. It receives and stores bile, produced by the liver, via the common hepatic duct, and releases it via the common bile duct into the duodenum, where the bile helps in the digestion of fats.

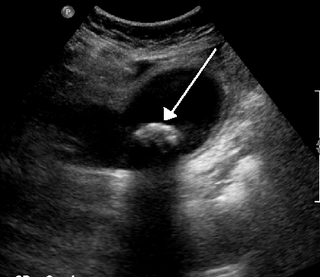
A gallstone is a stone formed within the gallbladder from precipitated bile components. The term cholelithiasis may refer to the presence of gallstones or to any disease caused by gallstones, and choledocholithiasis refers to the presence of migrated gallstones within bile ducts.
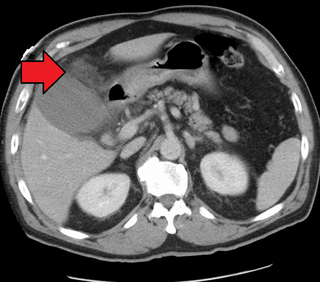
Cholecystitis is inflammation of the gallbladder. Symptoms include right upper abdominal pain, pain in the right shoulder, nausea, vomiting, and occasionally fever. Often gallbladder attacks precede acute cholecystitis. The pain lasts longer in cholecystitis than in a typical gallbladder attack. Without appropriate treatment, recurrent episodes of cholecystitis are common. Complications of acute cholecystitis include gallstone pancreatitis, common bile duct stones, or inflammation of the common bile duct.

Cholecystectomy is the surgical removal of the gallbladder. Cholecystectomy is a common treatment of symptomatic gallstones and other gallbladder conditions. In 2011, cholecystectomy was the eighth most common operating room procedure performed in hospitals in the United States. Cholecystectomy can be performed either laparoscopically, or via an open surgical technique.
The bile acid sequestrants are a group of resins used to bind certain components of bile in the gastrointestinal tract. They disrupt the enterohepatic circulation of bile acids by combining with bile constituents and preventing their reabsorption from the gut. In general, they are classified as hypolipidemic agents, although they may be used for purposes other than lowering cholesterol. They are used in the treatment of chronic diarrhea due to bile acid malabsorption.
Malabsorption is a state arising from abnormality in absorption of food nutrients across the gastrointestinal (GI) tract. Impairment can be of single or multiple nutrients depending on the abnormality. This may lead to malnutrition and a variety of anaemias.
Functional gastrointestinal disorders (FGID), also known as disorders of gut–brain interaction, include a number of separate idiopathic disorders which affect different parts of the gastrointestinal tract and involve visceral hypersensitivity and motility disturbances.

Gastrointestinal diseases refer to diseases involving the gastrointestinal tract, namely the esophagus, stomach, small intestine, large intestine and rectum, and the accessory organs of digestion, the liver, gallbladder, and pancreas.

Common bile duct stone, also known as choledocholithiasis, is the presence of gallstones in the common bile duct (CBD). This condition can cause jaundice and liver cell damage. Treatments include choledocholithotomy and endoscopic retrograde cholangiopancreatography (ERCP).
The Rome process and Rome criteria are an international effort to create scientific data to help in the diagnosis and treatment of functional gastrointestinal disorders, such as irritable bowel syndrome, functional dyspepsia and rumination syndrome. The Rome diagnostic criteria are set forth by Rome Foundation, a not for profit 501(c)(3) organization based in Raleigh, North Carolina, United States.
Biliary colic, also known as symptomatic cholelithiasis, a gallbladder attack or gallstone attack, is when a colic occurs due to a gallstone temporarily blocking the cystic duct. Typically, the pain is in the right upper part of the abdomen, and can be severe. Pain usually lasts from 15 minutes to a few hours. Often, it occurs after eating a heavy meal, or during the night. Repeated attacks are common.

The biliary tract refers to the liver, gallbladder and bile ducts, and how they work together to make, store and secrete bile. Bile consists of water, electrolytes, bile acids, cholesterol, phospholipids and conjugated bilirubin. Some components are synthesized by hepatocytes ; the rest are extracted from the blood by the liver.

Gallbladder diseases are diseases involving the gallbladder and is closely linked to biliary disease, with the most common cause being gallstones (cholelithiasis).

Colesevelam is a bile acid sequestrant administered orally. It was developed by GelTex Pharmaceuticals and later acquired by Genzyme. It is marketed in the U.S. by Daiichi Sankyo under the brand name Welchol and elsewhere by Genzyme as Cholestagel. In Canada, it is marketed by Valeant as Lodalis.
Biliary dyskinesia is a disorder of some component of biliary part of the digestive system in which bile cannot physically move in the proper direction through the tubular biliary tract. It most commonly involves abnormal biliary tract peristalsis muscular coordination within the gallbladder in response to dietary stimulation of that organ to squirt the liquid bile through the common bile duct into the duodenum. Ineffective peristaltic contraction of that structure produces postprandial right upper abdominal pain (cholecystodynia) and almost no other problem. When the dyskinesia is localized at the biliary outlet into the duodenum just as increased tonus of that outlet sphincter of Oddi, the backed-up bile can cause pancreatic injury with abdominal pain more toward the upper left side. In general, biliary dyskinesia is the disturbance in the coordination of peristaltic contraction of the biliary ducts, and/or reduction in the speed of emptying of the biliary tree into the duodenum.

SeHCAT is a drug used in a clinical test to diagnose bile acid malabsorption.

Sphincter of Oddi dysfunction refers to a group of functional disorders leading to abdominal pain due to dysfunction of the Sphincter of Oddi: functional biliary sphincter of Oddi and functional pancreatic sphincter of Oddi disorder. The sphincter of Oddi is a sphincter muscle, a circular band of muscle at the bottom of the biliary tree which controls the flow of pancreatic juices and bile into the second part of the duodenum. The pathogenesis of this condition is recognized to encompass stenosis or dyskinesia of the sphincter of Oddi ; consequently the terms biliary dyskinesia, papillary stenosis, and postcholecystectomy syndrome have all been used to describe this condition. Both stenosis and dyskinesia can obstruct flow through the sphincter of Oddi and can therefore cause retention of bile in the biliary tree and pancreatic juice in the pancreatic duct.
Bile acid malabsorption (BAM), known also as bile acid diarrhea, is a cause of several gut-related problems, the main one being chronic diarrhea. It has also been called bile acid-induced diarrhea, cholerheic or choleretic enteropathy, bile salt diarrhea or bile salt malabsorption. It can result from malabsorption secondary to gastrointestinal disease, or be a primary disorder, associated with excessive bile acid production. Treatment with bile acid sequestrants is often effective. It is recognised as a disability in the United Kingdom under the Equality Act 2010
Biliary microlithiasis refers to the creation of small gallstones less than 3 mm in diameter in the biliary duct or gallbladder.

A biloma is a circumscribed abdominal collection of bile outside the biliary tree. It occurs when there is excess bile in the abdominal cavity. It can occur during or after a bile leak. There is an increased chance of a person developing biloma after having a gallbladder removal surgery, known as laparoscopic cholecystectomy. This procedure can be complicated by biloma with incidence of 0.3–2%. Other causes are liver biopsy, abdominal trauma, and, rarely, spontaneous perforation. The formation of biloma does not occur frequently. Biliary fistulas are also caused by injury to the bile duct and can result in the formation of bile leaks. Biliary fistulas are abnormal communications between organs and the biliary tract. Once diagnosed, they usually require drainage. The term "biloma" was first coined in 1979 by Gould and Patel. They discovered it in a case with extrahepatic bile leakage. The cause of this was trauma to the upper right quadrant of the abdomen. Originally, biloma was described as an "encapsulated collection" of extrahepatic bile. Biloma is now described as extrabiliary collections of bile that can be either intrahepatic or extrahepatic. The most common cause of biloma is trauma to the liver. There are other causes such as abdominal surgery, endoscopic surgery and percutaneous catheter drainage. Injury and abdominal trauma can cause damage to the biliary tree. The biliary tree is a system of vessels that direct secreations from the liver, gallbladder, and pancreas through a series of ducts into the duodenum. This can result in a bile leak which is a common cause of the formation of biloma. It is possible for biloma to be associated with mortality, though it is not common. Bile leaks occur in about one percent of causes.