In neuroscience, an F wave is one of several motor responses which may follow the direct motor response (M) evoked by electrical stimulation of peripheral motor or mixed nerves. F-waves are the second of two late voltage changes observed after stimulation is applied to the skin surface above the distal region of a nerve, in addition to the H-reflex which is a muscle reaction in response to electrical stimulation of innervating sensory fibers. Traversal of F-waves along the entire length of peripheral nerves between the spinal cord and muscle, allows for assessment of motor nerve conduction between distal stimulation sites in the arm and leg, and related motoneurons (MN's) in the cervical and lumbosacral cord. F-waves are able to assess both afferent and efferent loops of the alpha motor neuron in its entirety. As such, various properties of F-wave motor nerve conduction are analyzed in nerve conduction studies (NCS), and often used to assess polyneuropathies, resulting from states of neuronal demyelination and loss of peripheral axonal integrity.

The foot is an anatomical structure found in many vertebrates. It is the terminal portion of a limb which bears weight and allows locomotion. In many animals with feet, the foot is a separate organ at the terminal part of the leg made up of one or more segments or bones, generally including claws or nails.

The human leg, in the general word sense, is the entire lower limb of the human body, including the foot, thigh and even the hip or gluteal region. However, the definition in human anatomy refers only to the section of the lower limb extending from the knee to the ankle, also known as the crus. Legs are used for standing, and all forms of locomotion including recreational such as dancing, and constitute a significant portion of a person's mass. Female legs generally have greater hip anteversion and tibiofemoral angles, but shorter femur and tibial lengths than those in males.
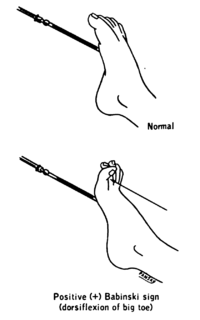
The plantar reflex is a reflex elicited when the sole of the foot is stimulated with a blunt instrument. The reflex can take one of two forms. In healthy adults, the plantar reflex causes a downward response of the hallux (flexion). An upward response (extension) of the hallux is known as the Babinski response or Babinski sign, named after the neurologist Joseph Babinski. The presence of the Babinski sign can identify disease of the spinal cord and brain in adults, and also exists as a primitive reflex in infants.

Human gait refers to locomotion achieved through the movement of human limbs. Human gait is defined as bipedal, biphasic forward propulsion of center of gravity of the human body, in which there are alternate sinuous movements of different segments of the body with least expenditure of energy. Different gait patterns are characterized by differences in limb-movement patterns, overall velocity, forces, kinetic and potential energy cycles, and changes in the contact with the surface. Human gaits are the various ways in which a human can move, either naturally or as a result of specialized training. Gait also refers to a religious approach to life, one can walk with a narrow or wide gait.
The withdrawal reflex is a spinal reflex intended to protect the body from damaging stimuli. The reflex rapidly coordinates the contractions of all the flexor muscles and the relaxations of the extensors in that limb causing sudden withdrawal from the potentially damaging stimulus. Spinal reflexes are often monosynaptic and are mediated by a simple reflex arc. A withdrawal reflex is mediated by a polysynaptic reflex resulting in the stimulation of many motor neurons in order to give a quick response.
The crossed extensor reflex or crossed extensor response or crossed extension reflex is a reflex in which the contralateral limb compensates for loss of support when the ipsilateral limb withdraws from painful stimulus in a withdrawal reflex. During a withdrawal reflex, the flexors in the withdrawing limb contract and the extensors relax, while in the other limb, the opposite occurs as part of the crossed extensor reflex. Besides shifting the body weight to the other side, the reflex pathway is also associated with leg coordination when walking by flexing muscle on one side, while extending muscle on the other side. This crossed extensor response is properly part of the withdrawal reflex.
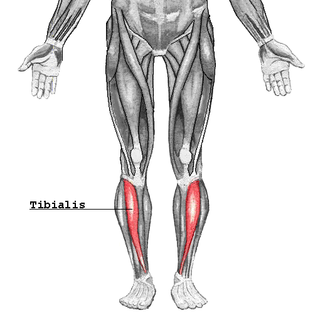
The tibialis anterior is a muscle in humans that originates along the upper two-thirds of the lateral (outside) surface of the tibia and inserts into the medial cuneiform and first metatarsal bones of the foot. It acts to dorsiflex and invert the foot. This muscle is mostly located near the shin.
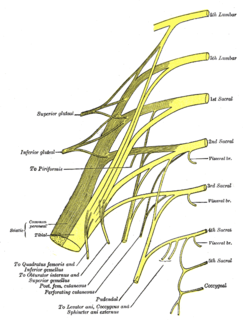
The tibial nerve is a branch of the sciatic nerve. The tibial nerve passes through the popliteal fossa to pass below the arch of soleus.

The plantaris is one of the superficial muscles of the superficial posterior compartment of the leg, one of the fascial compartments of the leg.

Foot drop is a gait abnormality in which the dropping of the forefoot happens due to weakness, irritation or damage to the common fibular nerve including the sciatic nerve, or paralysis of the muscles in the anterior portion of the lower leg. It is usually a symptom of a greater problem, not a disease in itself. Foot drop is characterized by inability or impaired ability to raise the toes or raise the foot from the ankle (dorsiflexion). Foot drop may be temporary or permanent, depending on the extent of muscle weakness or paralysis and it can occur in one or both feet. In walking, the raised leg is slightly bent at the knee to prevent the foot from dragging along the ground.

The vestibulospinal tract is a neural tract in the central nervous system. Specifically, it is a component of the extrapyramidal system and is classified as a component of the medial pathway. Like other descending motor pathways, the vestibulospinal fibers of the tract relay information from nuclei to motor neurons. The vestibular nuclei receive information through the vestibulocochlear nerve about changes in the orientation of the head. The nuclei relay motor commands through the vestibulospinal tract. The function of these motor commands is to alter muscle tone, extend, and change the position of the limbs and head with the goal of supporting posture and maintaining balance of the body and head.

The sole is the bottom of the foot.

Locomotor effects of shoes are the way in which the physical characteristics or components of shoes influence the locomotion neuromechanics of a person. Depending on the characteristics of the shoes, the effects are various, ranging from alteration in balance and posture, muscle activity of different muscles as measured by electromyography (EMG), and the impact force. There are many different types of shoes that exist, such as running, walking, loafers, high heels, sandals, slippers, work boots, dress shoes, and many more. However, a typical shoe will be composed of an insole, midsole, outsole, and heels, if any. In an unshod condition, where one is without any shoes, the locomotor effects are primarily observed in the heel strike patterns and resulting impact forces generated on the ground.

Spinal locomotion results from intricate dynamic interactions between a central program in lower thoracolumbar spine and proprioceptive feedback from body in the absence of central control by brain as in complete spinal cord injury (SCI). Following SCI, the spinal circuitry below the lesion site does not become silent rather it continues to maintain active and functional neuronal properties although in a modified manner.
Terrestrial locomotion by means of a running gait can be accomplished on level surfaces. However, in most outdoor environments an individual will experience terrain undulations requiring uphill running. Similar conditions can be mimicked in a controlled environment on a treadmill also. Additionally, running on inclines is used by runners, both distance and sprinter, to improve cardiovascular conditioning and lower limb strength.

Central pattern generators are biological neural networks organized to produce any rhythmic output without requiring a rhythmic input. In mammals, locomotor CPGs are organized in the lumbar and cervical segments of the spinal cord, and are used to control rhythmic muscle output in the arms and legs. Certain areas of the brain initiate the descending neural pathways that ultimately control and modulate the CPG signals. In addition to this direct control, there exist different feedback loops that coordinate the limbs for efficient locomotion and allow for the switching of gaits under appropriate circumstances.

As originally proposed by Enoka, neuromechanics is a field of study that combines concepts from biomechanics and neurophysiology to study human movement. Neuromechanics examines the combined roles of the skeletal, muscular, and nervous systems and how they interact to produce the motion required to complete a motor task.
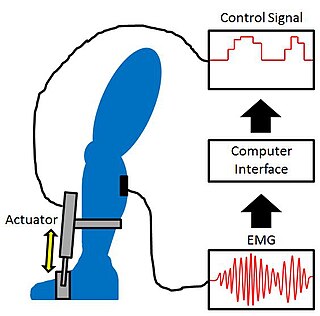
Proportional myoelectric control can be used to activate robotic lower limb exoskeletons. A proportional myoelectric control system utilizes a microcontroller or computer that inputs electromyography (EMG) signals from sensors on the leg muscle(s) and then activates the corresponding joint actuator(s) proportionally to the EMG signal.









