Related Research Articles

Physical therapy (PT), also known as physiotherapy, is a healthcare profession, as well as the care provided by physical therapists who promote, maintain, or restore health through patient education, physical intervention, disease prevention, and health promotion. Physical therapist is the term used for such professionals in the United States, and physiotherapist is the term used in many other countries.
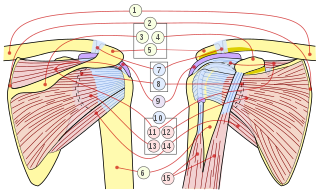
The rotator cuff is a group of muscles and their tendons that act to stabilize the human shoulder and allow for its extensive range of motion. Of the seven scapulohumeral muscles, four make up the rotator cuff. The four muscles are:
A mechanoreceptor, also called mechanoceptor, is a sensory receptor that responds to mechanical pressure or distortion. Mechanoreceptors are innervated by sensory neurons that convert mechanical pressure into electrical signals that, in animals, are sent to the central nervous system.
Manual therapy, or manipulative therapy, is a part of Physiotherapy, it is a physical treatment primarily used by physical therapists, occupational therapists to treat musculoskeletal pain and disability; it mostly includes kneading and manipulation of muscles, joint mobilization and joint manipulation. It is also used by Rolfers, massage therapists, athletic trainers, osteopaths, and physicians.

Adhesive capsulitis (AC), also known as frozen shoulder, is a condition associated with shoulder pain and stiffness. It is a common shoulder ailment that is marked by pain and a loss of range of motion, particularly in external rotation. There is a loss of the ability to move the shoulder, both voluntarily and by others, in multiple directions. The shoulder itself, however, does not generally hurt significantly when touched. Muscle loss around the shoulder may also occur. Onset is gradual over weeks to months. Complications can include fracture of the humerus or biceps tendon rupture.

Spinal manipulation is an intervention performed on synovial joints of the spine, including the z-joints, the atlanto-occipital, atlanto-axial, lumbosacral, sacroiliac, costotransverse and costovertebral joints. It is typically applied with therapeutic intent, most commonly for the treatment of low back pain.

Traction is a set of mechanisms for straightening broken bones or relieving pressure on the spine and skeletal system. There are two types of traction: skin traction and skeletal traction. They are used in orthopedic medicine.
Counterstrain is a technique used in osteopathic medicine, osteopathy, physical therapy, massage therapy, and chiropractic to treat somatic dysfunction. It is a system of diagnosis and treatment that uses tender points, which are produced by trauma, inflammation, postural strain, or disease, to identify structures to manipulate. The manipulation uses light pressure to decompress the local nociceptors and mechanoreceptors responsible for the sensation of pain, returning central sensitization to its normal state. This technique extends Strain-counterstrain, a technique inhibits the reflexes by putting the tissues in a position of ease directly opposite to that of the reflex. Strain-counterstrain is also known as the Jones technique,, and spontaneous release by position. Counterstrain was developed by Lawrence Jones in 1955 and was originally called “Spontaneous Release by Positioning,” before being termed “strain-counterstrain.”
Joint manipulation is a type of passive movement of a skeletal joint. It is usually aimed at one or more 'target' synovial joints with the aim of achieving a therapeutic effect.
Manipulation under anesthesia (MUA) or fibrosis release procedures is a multidisciplinary, chronic pain-related manual therapy modality which is used for the purpose of improving articular and soft tissue movement. This is accomplished by way of a combination of controlled joint mobilization/manipulation and myofascial release techniques. MUA is used by osteopathic/orthopedic physicians, chiropractors and specially trained physicians. It aims to break up adhesions on or around spinal joints or extremity joints to which a restricted range of motion can be painful and limit function. Failed attempts at other standard conservative treatment methods, over a sufficient time-frame, is one of the principal patient qualifiers.

Patellofemoral pain syndrome is knee pain as a result of problems between the kneecap and the femur. The pain is generally in the front of the knee and comes on gradually. Pain may worsen with sitting down with a bent knee for long periods of time, excessive use, or climbing and descending stairs.
Spinal mobilization is a type of passive movement of a spinal segment or region. It is usually performed with the aim of achieving a therapeutic effect.

The somatosensory system, or somatic sensory system is a subset of the sensory nervous system. It has two subdivisions, one for the detection of mechanosensory information related to touch, and the other for the nociception detection of pain and temperature. The main functions of the somatosensory system are the perception of external stimuli, the perception of internal stimuli, and the regulation of body position and balance (proprioception).
The terms "arthrokinetic reflex" was coined by medical researchers at the University of Pittsburgh's Medical School, department of Physiology, in 1956 to refer to the way in which joint movement can reflexively cause muscle activation or inhibition.

Spinal locomotion results from intricate dynamic interactions between a central program in lower thoracolumbar spine and proprioceptive feedback from body in the absence of central control by brain as in complete spinal cord injury (SCI). Following SCI, the spinal circuitry below the lesion site does not become silent; rather, it continues to maintain active and functional neuronal properties, although in a modified manner.
Dynasplint Systems, Incorporated (DSI) is a company that designs, manufactures and sells dynamic splints that are used for range of motion rehabilitation. The corporate headquarters are located in Severna Park, Maryland and it is considered a major employer in Anne Arundel County. Products are Made in the US in Stevensville, Maryland. There is a national sales force throughout the US as well as a presence in Canada and Europe.

Watsu is a form of aquatic bodywork used for deep relaxation and passive aquatic therapy. Watsu is characterized by one-on-one sessions in which a practitioner or therapist gently cradles, moves, stretches, and massages a receiver in chest-deep warm water.
Passive accessory intervertebral movements (PAIVM) refers to a spinal physical therapy assessment and treatment technique developed by Geoff Maitland. The purpose of PAIVM is to assess the amount and quality of movement at various intervertebral levels, and to treat pain and stiffness of the cervical and lumbar spine.
Passive physiological intervertebral movements (PPIVM) refers to a spinal physical therapy assessment and treatment technique developed by Geoff Maitland used to assess intervertebral movement at a single joint, and to mobilise neck stiffness.
Natural apophyseal glides (NAGS) refers to a spinal physical therapy treatment technique developed by Brian Mulligan.
References
- ↑ "Educational Standards In Orthopaedic Manipulative Therapy" (PDF). International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT) INC. Archived (PDF) from the original on 17 November 2023. Retrieved 6 July 2024.
- ↑ Guide to Physical Therapist Practice 3.0. Alexandria, VA: American Physical Therapy Association; 2014.
- ↑ Maitland, G.D. Peripheral Manipulation 2nd ed. Butterworths, London, 1977. Maitland, G.D. Vertebral Manipulation 5th ed. Butterworths, London, 1986.
