
An advance healthcare directive, also known as living will, personal directive, advance directive, medical directive or advance decision, is a legal document in which a person specifies what actions should be taken for their health if they are no longer able to make decisions for themselves because of illness or incapacity. In the U.S. it has a legal status in itself, whereas in some countries it is legally persuasive without being a legal document.
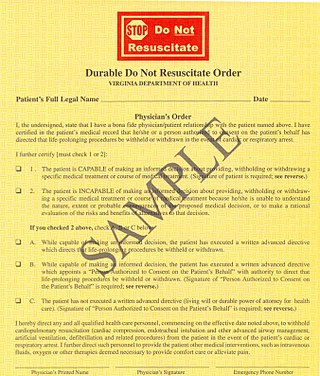
A do-not-resuscitate order (DNR), also known as Do Not Attempt Resuscitation (DNAR), Do Not Attempt Cardiopulmonary Resuscitation (DNACPR), no code or allow natural death, is a medical order, written or oral depending on the jurisdiction, indicating that a person should not receive cardiopulmonary resuscitation (CPR) if that person's heart stops beating. Sometimes these decisions and the relevant documents also encompass decisions around other critical or life-prolonging medical interventions. The legal status and processes surrounding DNR orders vary in different polities. Most commonly, the order is placed by a physician based on a combination of medical judgement and patient involvement.

Life support comprises the treatments and techniques performed in an emergency in order to support life after the failure of one or more vital organs. Healthcare providers and emergency medical technicians are generally certified to perform basic and advanced life support procedures; however, basic life support is sometimes provided at the scene of an emergency by family members or bystanders before emergency services arrive. In the case of cardiac injuries, cardiopulmonary resuscitation is initiated by bystanders or family members 25% of the time. Basic life support techniques, such as performing CPR on a victim of cardiac arrest, can double or even triple that patient's chance of survival. Other types of basic life support include relief from choking, staunching of bleeding by direct compression and elevation above the heart, first aid, and the use of an automated external defibrillator.
In medicine, specifically in end-of-life care, palliative sedation is the palliative practice of relieving distress in a terminally ill person in the last hours or days of a dying person's life, usually by means of a continuous intravenous or subcutaneous infusion of a sedative drug, or by means of a specialized catheter designed to provide comfortable and discreet administration of ongoing medications via the rectal route.
Terminal illness or end-stage disease is a disease that cannot be cured or adequately treated and is expected to result in the death of the patient. This term is more commonly used for progressive diseases such as cancer, dementia or advanced heart disease than for injury. In popular use, it indicates a disease that will progress until death with near absolute certainty, regardless of treatment. A patient who has such an illness may be referred to as a terminal patient, terminally ill or simply as being terminal. There is no standardized life expectancy for a patient to be considered terminal, although it is generally months or less. Life expectancy for terminal patients is a rough estimate given by the physician based on previous data and does not always reflect true longevity. An illness which is lifelong but not fatal is a chronic condition.
Futile medical care is the continued provision of medical care or treatment to a patient when there is no reasonable hope of a cure or benefit.

The Vial of Life, also known as Vial of L.I.F.E. is a program that allows individuals to have their complete medical information ready in their home for emergency personnel to reference during an emergency. The program is used to provide the patient's medical information when a patient is not able to speak or remember this information. Vial of Life programs are commonly used by senior citizens and promoted by senior center organizations, fire departments, and other community organizations.
In the field of medicine, a healthcare proxy is a document with which a patient appoints an agent to legally make healthcare decisions on behalf of the patient, when the patient is incapable of making and executing the healthcare decisions stipulated in the proxy. Once the healthcare proxy is effective, the agent continues making healthcare decisions as long as the primary individual is legally competent to decide. Moreover, in legal-administrative functions, the healthcare proxy is a legal instrument akin to a "springing" healthcare power of attorney. The proxy must declare the healthcare agent who will gain durable power attorney. This document also notifies of the authority given from the principal to the agent and states the limitations of this authority.
Involuntary Euthanasia is currently illegal in all 50 states of the United States. Assisted suicide is legal in 10 jurisdictions in the US: Washington, D.C. and the states of California, Colorado, Oregon, Vermont, New Mexico, Maine, New Jersey, Hawaii, and Washington. The status of assisted suicide is disputed in Montana, though currently authorized per the Montana Supreme Court's ruling in Baxter v. Montana that "nothing in Montana Supreme Court precedent or Montana statutes [indicates] that physician aid in dying is against public policy."
The philosophy of healthcare is the study of the ethics, processes, and people which constitute the maintenance of health for human beings. For the most part, however, the philosophy of healthcare is best approached as an indelible component of human social structures. That is, the societal institution of healthcare can be seen as a necessary phenomenon of human civilization whereby an individual continually seeks to improve, mend, and alter the overall nature and quality of their life. This perennial concern is especially prominent in modern political liberalism, wherein health has been understood as the foundational good necessary for public life.

Hospice care is a type of health care that focuses on the palliation of a terminally ill patient's pain and symptoms and attending to their emotional and spiritual needs at the end of life. Hospice care prioritizes comfort and quality of life by reducing pain and suffering. Hospice care provides an alternative to therapies focused on life-prolonging measures that may be arduous, likely to cause more symptoms, or are not aligned with a person's goals.
The Family Health Care Decisions Act is a statute adopted in New York state in 2010 that had been pending before the legislature since 1994. The statute was approved by the New York State Senate in July, 2009. The legislation was introduced by state senator Thomas Duane of Manhattan. It was signed into law by Gov. David Paterson on March 16, 2010.
Betancourt v. Trinitas Hospital, 1 A.3d 823 (2010), is a New Jersey legal case concerning whether a hospital may unilaterally refuse care to a patient on the grounds that it is futile to prolong the person's life because there is little chance that the condition will improve. It has become the focal point of the ongoing debate surrounding denial of care among professional bioethicists.
The Texas Advance Directives Act (1999), also known as the Texas Futile Care Law, describes certain provisions that are now Chapter 166 of the Texas Health & Safety Code. Controversy over these provisions mainly centers on Section 166.046, Subsection (e), which allows a health care facility to discontinue life-sustaining treatment ten days after giving written notice if the continuation of life-sustaining treatment is considered futile care by the treating medical team.
Allow Natural Death (AND) is a medical term defining the use of life-extending measures such as cardiopulmonary resuscitation (CPR). These orders emphasize patient comfort and pain management instead of life extension. Currently, American medical communities utilize "do not resuscitate," (DNR) orders to define patients' medical wishes. Those who propose to replace DNR with AND posit that DNR orders are ambiguous and require complex understanding between several parties, while AND orders are clearer. Proponents of replacing DNR with AND believe that AND terminology is more ethically conscientious DNR terminology. Research has been conducted regarding participant preference for AND vs. DNR terminology. The ease with which the terminology change can be practically incorporated depends on many factors such as costs and staff reeducation.
POLST is an approach to improving end-of-life care in the United States, encouraging providers to speak with the severely ill and create specific medical orders to be honored by health care workers during a medical crisis. POLST began in Oregon in 1991 and currently exists in 46 states; some of the 46 states have the program in development. The POLST document is a standardized, portable, brightly colored single page medical order that documents a conversation between a provider and an individual with a serious illness or frailty towards the end of life. A POLST form allows emergency medical services to provide treatment that the individual prefers before possibly transporting to an emergency facility.
Slow code refers to the practice in a hospital or other medical centre to purposely respond slowly or incompletely to a patient in cardiac arrest, particularly in situations for which cardiopulmonary resuscitation (CPR) is thought to be of no medical benefit by the medical staff. The related term show code refers to the practice of a medical response that is medically futile, but is attempted for the benefit of the patient's family and loved ones. However, the terms are often used interchangeably.
Maternal somatic support after brain death occurs when a brain dead patient is pregnant and their body is kept alive to deliver a fetus. It occurs very rarely internationally. Even among brain dead patients, in a U.S. study of 252 brain dead patients from 1990–96, only 5 (2.8%) cases involved pregnant women between 15 and 45 years of age.
In the law of England and Wales, best interest decisions are decisions made on behalf of people who do not have mental capacity to make them for themselves at the time the decision needs to be taken. Someone who has the capacity to make a decision is said to be "capacitous". Since 2007, there has been a dedicated court with jurisdiction over mental capacity: the Court of Protection, although it mostly deals with adults. Most applications to make decisions on behalf of a child are still dealt with by the Family Court.
ReSPECT stands for Recommended Summary Plan for Emergency Care and Treatment. It is an emergency care and treatment plan (ECTP) used in parts of the United Kingdom, in which personalized recommendations for future emergency clinical care and treatment are created through discussion between health care professionals and a person. These recommendations are then documented on a ReSPECT form.

{kind=link}