Related Research Articles

The leg is the entire lower limb of the human body, including the foot, thigh or sometimes even the hip or buttock region. The major bones of the leg are the femur, tibia, and adjacent fibula. There are 60 leg bones in each leg.
Articles related to anatomy include:

In anatomy, the thigh is the area between the hip (pelvis) and the knee. Anatomically, it is part of the lower limb.

The sciatic nerve, also called the ischiadic nerve, is a large nerve in humans and other vertebrate animals. It is the largest branch of the sacral plexus and runs alongside the hip joint and down the lower limb. It is the longest and widest single nerve in the human body, going from the top of the leg to the foot on the posterior aspect. The sciatic nerve has no cutaneous branches for the thigh. This nerve provides the connection to the nervous system for the skin of the lateral leg and the whole foot, the muscles of the back of the thigh, and those of the leg and foot. It is derived from spinal nerves L4 to S3. It contains fibres from both the anterior and posterior divisions of the lumbosacral plexus.
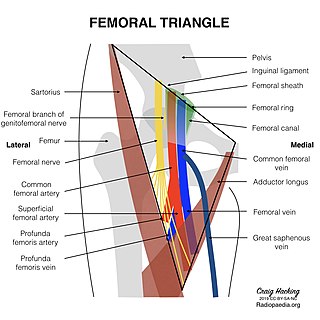
The femoral triangle is an anatomical region of the upper third of the thigh. It is a subfascial space which appears as a triangular depression below the inguinal ligament when the thigh is flexed, abducted and laterally rotated.

In human anatomy, the fibularis longus is a superficial muscle in the lateral compartment of the leg. It acts to tilt the sole of the foot away from the midline of the body (eversion) and to extend the foot downward away from the body at the ankle.

In humans and some other mammals, the soleus is a powerful muscle in the back part of the lower leg. It runs from just below the knee to the heel and is involved in standing and walking. It is closely connected to the gastrocnemius muscle, and some anatomists consider this combination to be a single muscle, the triceps surae. Its name is derived from the Latin word "solea", meaning "sandal".
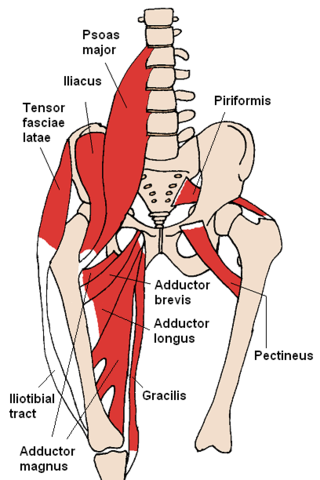
The gracilis muscle is the most superficial muscle on the medial side of the thigh. It is thin and flattened, broad above, narrow and tapering below.

The flexor digitorum longus muscle or flexor digitorum communis longus is situated on the tibial side of the leg. At its origin it is thin and pointed, but it gradually increases in size as it descends. It serves to flex the second, third, fourth, and fifth toes.

In human anatomy, the fibularis brevis is a muscle that lies underneath the fibularis longus within the lateral compartment of the leg. It acts to tilt the sole of the foot away from the midline of the body (eversion) and to extend the foot downward away from the body at the ankle.
The common fibular nerve is a nerve in the lower leg that provides sensation over the posterolateral part of the leg and the knee joint. It divides at the knee into two terminal branches: the superficial fibular nerve and deep fibular nerve, which innervate the muscles of the lateral and anterior compartments of the leg respectively. When the common fibular nerve is damaged or compressed, foot drop can ensue.

The superficial fibular nerve is a mixed nerve that provides motor innervation to the fibularis longus and fibularis brevis muscles, and sensory innervation to skin over the antero-lateral aspect of the leg along with the greater part of the dorsum of the foot.
The deep fibular nerve begins at the bifurcation of the common fibular nerve between the fibula and upper part of the fibularis longus, passes infero-medially, deep to the extensor digitorum longus, to the anterior surface of the interosseous membrane, and comes into relation with the anterior tibial artery above the middle of the leg; it then descends with the artery to the front of the ankle-joint, where it divides into a lateral and a medial terminal branch.

The popliteal fossa is a shallow depression located at the back of the knee joint. The bones of the popliteal fossa are the femur and the tibia. Like other flexion surfaces of large joints, it is an area where blood vessels and nerves pass relatively superficially, and with an increased number of lymph nodes.

In humans, the sole of the foot is anatomically referred to as the plantar aspect.
The saphenous nerve is the largest cutaneous branch of the femoral nerve. It is derived from the lumbar plexus (L3-L4). It is a strictly sensory nerve, and has no motor function. It commences in the proximal (upper) thigh and travels along the adductor canal. Upon exiting the adductor canal, the saphenous nerve terminates by splitting into two terminal branches: the sartorial nerve, and the infrapatellar nerve. The saphenous nerve is responsible for providing sensory innervation to the skin of the anteromedial leg.

The anterior compartment of the leg is a fascial compartment of the lower leg. It contains muscles that produce dorsiflexion and participate in inversion and eversion of the foot, as well as vascular and nervous elements, including the anterior tibial artery and veins and the deep fibular nerve.

The following outline is provided as an overview of and topical guide to human anatomy:
The subsartorial plexus is a plexus of nerves that is located under the sartorius muscle.

In anatomy, the fibular artery, also known as the peroneal artery, supplies blood to the lateral compartment of the leg. It arises from the tibial-fibular trunk.
References
- Gray's Anatomy: The Anatomical Basis of Clinical Practice, Expert Consult, 40e. By Susan Standring, PhD, DSc, Emeritus Professor of Anatomy, Head of Anatomy and Human Sciences, King's College London, London, UK. 9780443066849
- ↑ "AO Surgery Reference". AO Foundation. Retrieved 16 October 2015.
- ↑ Faure Walker, Nicholas; Nair, Rajesh; Anderson, Chris (September 2015). "Re: Gunnar Steineck, Anders Bjartell, Jonas Hugosson, et al. Degree of Preservation of the Neurovascular Bundles During Radical Prostatectomy and Urinary Continence 1 Year after Surgery. Eur Urol 2015;67:559–68". European Urology. 68 (3): e63. doi:10.1016/j.eururo.2015.04.014. PMID 25913067.
- ↑ "The Patrick C. Walsh Prostate Cancer Research Fund: The Winning Vision Continues".