Related Research Articles

Interferons are a group of signaling proteins made and released by host cells in response to the presence of several viruses. In a typical scenario, a virus-infected cell will release interferons causing nearby cells to heighten their anti-viral defenses.
Coxsackie A virus (CAV) is a cytolytic Coxsackievirus of the Picornaviridae family, an enterovirus.

Antiviral drugs are a class of medication used for treating viral infections. Most antivirals target specific viruses, while a broad-spectrum antiviral is effective against a wide range of viruses. Antiviral drugs are one class of antimicrobials, a larger group which also includes antibiotic, antifungal and antiparasitic drugs, or antiviral drugs based on monoclonal antibodies. Most antivirals are considered relatively harmless to the host, and therefore can be used to treat infections. They should be distinguished from virucides, which are not medication but deactivate or destroy virus particles, either inside or outside the body. Natural virucides are produced by some plants such as eucalyptus and Australian tea trees.
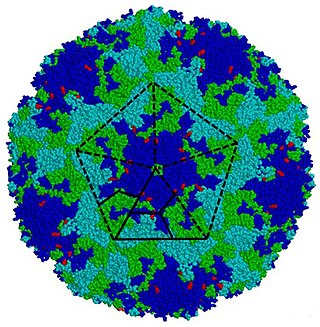
Coxsackie B4 virus are enteroviruses that belong to the Picornaviridae family. These viruses can be found worldwide. They are positive-sense, single-stranded, non-enveloped RNA viruses with icosahedral geometry. Coxsackieviruses have two groups, A and B, each associated with different diseases. Coxsackievirus group A is known for causing hand-foot-and-mouth diseases while Group B, which contains six serotypes, can cause a varying range of symptoms like gastrointestinal distress myocarditis. Coxsackievirus B4 has a cell tropism for natural killer cells and pancreatic islet cells. Infection can lead to beta cell apoptosis which increases the risk of insulitis.

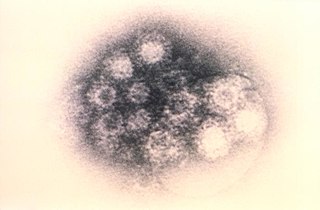
Coxsackieviruses are a few related enteroviruses that belong to the Picornaviridae family of nonenveloped, linear, positive-sense single-stranded RNA viruses, as well as its genus Enterovirus, which also includes poliovirus and echovirus. Enteroviruses are among the most common and important human pathogens, and ordinarily its members are transmitted by the fecal–oral route. Coxsackieviruses share many characteristics with poliovirus. With control of poliovirus infections in much of the world, more attention has been focused on understanding the nonpolio enteroviruses such as coxsackievirus.
Coxsackie B is a group of six serotypes of coxsackievirus (CVB1-CVB6), a pathogenic enterovirus, that trigger illness ranging from gastrointestinal distress to full-fledged pericarditis and myocarditis.

Myocarditis, also known as inflammatory cardiomyopathy, is an acquired cardiomyopathy due to inflammation of the heart muscle. Symptoms can include shortness of breath, chest pain, decreased ability to exercise, and an irregular heartbeat. The duration of problems can vary from hours to months. Complications may include heart failure due to dilated cardiomyopathy or cardiac arrest.

Adenoviruses are medium-sized, nonenveloped viruses with an icosahedral nucleocapsid containing a double-stranded DNA genome. Their name derives from their initial isolation from human adenoids in 1953.
Enterovirus is a genus of positive-sense single-stranded RNA viruses associated with several human and mammalian diseases. Enteroviruses are named by their transmission-route through the intestine.
Viral pathogenesis is the study of the process and mechanisms by which viruses cause diseases in their target hosts, often at the cellular or molecular level. It is a specialized field of study in virology.

Herpes simplex virus1 and 2, also known by their taxonomic names Human alphaherpesvirus 1 and Human alphaherpesvirus 2, are two members of the human Herpesviridae family, a set of viruses that produce viral infections in the majority of humans. Both HSV-1 and HSV-2 are very common and contagious. They can be spread when an infected person begins shedding the virus.
Entry inhibitors, also known as fusion inhibitors, are a class of antiviral drugs that prevent a virus from entering a cell, for example, by blocking a receptor. Entry inhibitors are used to treat conditions such as HIV and hepatitis D.

Pleconaril (Picovir) is an antiviral drug that was being developed by Schering-Plough for prevention of asthma exacerbations and common cold symptoms in patients exposed to picornavirus respiratory infections. Pleconaril, administered either orally or intranasally, is active against viruses in the Picornaviridae family, including Enterovirus and Rhinovirus. It has shown useful activity against the dangerous enterovirus D68.
CD4 immunoadhesin is a recombinant fusion protein consisting of a combination of CD4 and the fragment crystallizable region, similarly known as immunoglobulin. It belongs to the antibody (Ig) gene family. CD4 is a surface receptor for human immunodeficiency virus (HIV). The CD4 immunoadhesin molecular fusion allow the protein to possess key functions from each independent subunit. The CD4 specific properties include the gp120-binding and HIV-blocking capabilities. Properties specific to immunoglobulin are the long plasma half-life and Fc receptor binding. The properties of the protein means that it has potential to be used in AIDS therapy as of 2017. Specifically, CD4 immunoadhesin plays a role in antibody-dependent cell-mediated cytotoxicity (ADCC) towards HIV-infected cells. While natural anti-gp120 antibodies exhibit a response towards uninfected CD4-expressing cells that have a soluble gp120 bound to the CD4 on the cell surface, CD4 immunoadhesin, however, will not exhibit a response. One of the most relevant of these possibilities is its ability to cross the placenta.

Coxsackievirus and adenovirus receptor (CAR) is a protein that in humans is encoded by the CXADR gene. The protein encoded by this gene is a type I membrane receptor for group B coxsackie viruses and subgroup C adenoviruses. CAR protein is expressed in several tissues, including heart, brain, and, more generally, epithelial and endothelial cells. In cardiac muscle, CAR is localized to intercalated disc structures, which electrically and mechanically couple adjacent cardiomyocytes. CAR plays an important role in the pathogenesis of myocarditis, dilated cardiomyopathy, and in arrhythmia susceptibility following myocardial infarction or myocardial ischemia. In addition, an isoform of CAR (CAR-SIV) has been recently identified in the cytoplasm of pancreatic beta cells. It's been suggested that CAR-SIV resides in the insulin secreting granules and might be involved in the virus infection of these cells.

Influenza, commonly known as "the flu", is an infectious disease caused by influenza viruses. Symptoms range from mild to severe and often include fever, runny nose, sore throat, muscle pain, headache, coughing, and fatigue. These symptoms begin from one to four days after exposure to the virus and last for about 2–8 days. Diarrhea and vomiting can occur, particularly in children. Influenza may progress to pneumonia, which can be caused by the virus or by a subsequent bacterial infection. Other complications of infection include acute respiratory distress syndrome, meningitis, encephalitis, and worsening of pre-existing health problems such as asthma and cardiovascular disease.
A neutralizing antibody (NAb) is an antibody that defends a cell from a pathogen or infectious particle by neutralizing any effect it has biologically. Neutralization renders the particle no longer infectious or pathogenic. Neutralizing antibodies are part of the humoral response of the adaptive immune system against viruses, intracellular bacteria and microbial toxin. By binding specifically to surface structures (antigen) on an infectious particle, neutralizing antibodies prevent the particle from interacting with its host cells it might infect and destroy.
Coxsackieviruses-induced cardiomyopathy are positive-stranded RNA viruses in picornavirus family and the genus enterovirus, acute enterovirus infections such as Coxsackievirus B3 have been identified as the cause of virally induced acute myocarditis, resulting in dilated cardiomyopathy. Dilated cardiomyopathy in humans can be caused by multiple factors including hereditary defects in the cytoskeletal protein dystrophin in Duchenne muscular dystrophy (DMD) patients). A heart that undergoes dilated cardiomyopathy shows unique enlargement of ventricles, and thinning of the ventricular wall that may lead to heart failure. In addition to the genetic defects in dystrophin or other cytoskeletal proteins, a subset of dilated cardiomyopathy is linked to enteroviral infection in the heart, especially coxsackievirus B. Enterovirus infections are responsible for about 30% of the cases of acquired dilated cardiomyopathy in humans.
Viral cardiomyopathy occurs when viral infections cause myocarditis with a resulting thickening of the myocardium and dilation of the ventricles. These viruses include Coxsackie B and adenovirus, echoviruses, influenza H1N1, Epstein–Barr virus, rubella, varicella, mumps, measles, parvoviruses, yellow fever, dengue fever, polio, rabies and the viruses that cause hepatitis A and C, as well as COVID-19, which has been seen to cause this in persons otherwise thought to have a "low risk" of the virus's effects.
Heart problems are more common in people with HIV/AIDS. Those with left ventricular dysfunction have a median survival of 101 days as compared to 472 days in people with AIDS with healthy hearts. HIV is a major cause of cardiomyopathy. The most common type of HIV induced cardiomyopathy is dilated cardiomyopathy also known as eccentric ventricular hypertrophy which leads to impaired contraction of the ventricles due to volume overload. The annual incidence of HIV associated dilated cardiomyopathy was 15.9/1000 before the introduction of highly active antiretroviral therapy (HAART). However, in 2014, a study found that 17.6% of HIV patients have dilated cardiomyopathy (176/1000) meaning the incidence has greatly increased.
References
- 1 2 3 4 5 Werk D, Pinkert S, Heim A, et al. (September 2009). "Combination of soluble coxsackievirus-adenovirus receptor and anti-coxsackievirus siRNAs exerts synergistic antiviral activity against coxsackievirus B3". Antiviral Res. 83 (3): 298–306. doi:10.1016/j.antiviral.2009.07.002. PMID 19591879.
- 1 2 3 Goodfellow IG, Evans DJ, Blom AM, et al. (September 2005). "Inhibition of coxsackie B virus infection by soluble forms of its receptors: binding affinities, altered particle formation, and competition with cellular receptors". J. Virol. 79 (18): 12016–24. doi:10.1128/JVI.79.18.12016-12024.2005. PMC 1212587 . PMID 16140777.
- ↑ Yanagawa B, Spiller OB, Proctor DG, et al. (April 2004). "Soluble recombinant coxsackievirus and adenovirus receptor abrogates coxsackievirus b3-mediated pancreatitis and myocarditis in mice". J. Infect. Dis. 189 (8): 1431–9. doi: 10.1086/382598 . PMID 15073680.
- ↑ Woodruff JF (November 1980). "Viral myocarditis. A review". Am. J. Pathol. 101 (2): 425–84. PMC 1903609 . PMID 6254364.
- 1 2 Onyimba JA, Coronado MJ, Garton AE, et al. (2011). "The innate immune response to coxsackievirus B3 predicts progression to cardiovascular disease and heart failure in male mice". Biol Sex Differ. 2: 2. doi: 10.1186/2042-6410-2-2 . PMC 3049118 . PMID 21338512.
- ↑ Herzum M, Ruppert V, Küytz B, Jomaa H, Nakamura I, Maisch B (July 1994). "Coxsackievirus B3 infection leads to cell death of cardiac myocytes". J. Mol. Cell. Cardiol. 26 (7): 907–13. doi:10.1006/jmcc.1994.1108. PMID 7966359.
- ↑ Fechner H, Pinkert S, Geisler A, Poller W, Kurreck J (2011). "Pharmacological and biological antiviral therapeutics for cardiac coxsackievirus infections". Molecules. 16 (10): 8475–503. doi: 10.3390/molecules16108475 . PMC 6264230 . PMID 21989310.
- ↑ Milstone AM, Petrella J, Sanchez MD, Mahmud M, Whitbeck JC, Bergelson JM (January 2005). "Interaction with coxsackievirus and adenovirus receptor, but not with decay-accelerating factor (DAF), induces A-particle formation in a DAF-binding coxsackievirus B3 isolate". J. Virol. 79 (1): 655–60. doi:10.1128/JVI.79.1.655-660.2005. PMC 538729 . PMID 15596863.